
Naveedullah Khan ( National Institute of Cardiovascular Diseases, Karachi.Pakistan. )
Qurban Ali Rahu ( National Institute of Cardiovascular Diseases, Karachi.Pakistan. )
Habiba Tasneem ( National Institute of Cardiovascular Diseases, Karachi.Pakistan. )
HaMuhammad Ishaq ( National Institute of Cardiovascular Diseases, Karachi.Pakistan. )
Muhammad Tariq Farman ( National Institute of Cardiovascular Diseases, Karachi.Pakistan. )
Jawaid Akbar Sial ( National Institute of Cardiovascular Diseases, Karachi.Pakistan. )
June 2010, Volume 60, Issue 6
Original Article
Abstract
Objective: To determine the frequency of Left Atrial thrombus in patients suffering from severe mitral stenosis with atrial fibrillation.
Methods: A cross sectional descriptive type study was conducted in the Echocardiography department of the National Institute of Cardio Vascular Diseases (NICVD) Karachi from October 1, 2007 to March 17, 2008. A total of 100 consecutive adult patients with severe Mitral stenosis (MS) and Atrial Fibrillation (AF) were included in this study. 12-lead Electrocardiography was done once clinical and echocardiographic features revealed Sever MS. Patients with signs of AF were selected and Transthoracic Echocardiography (TTE) was obtained to detect Left Atrial Thrombus. Transesophageal echocardiography (TEE) was performed whenever thrombus could not be found with TTE and / or nature of the mass could not be confirmed.
Results: Among 100 patients studied; there were 52 males and 48 females. TTE was performed in all patients and LA thrombi were detected in 24% patients. TEE was performed in remaining 76% patients and additional 14 patients with LA thrombi were detected in this subgroup. Therefore a total of 38% of the patients with LA thrombi were documented. Among them, 6% had clots in LA body while LA appendage clots were found in 32% of patients. Left atrial dimension was found to be relevant (P-value = 0.004) with the presence of thrombus in patients with severe mitral stenosis associated with atrial fibrillation. Left atrial spontaneous echo contrast (LASEC) was found in 54% of patients but it was not found to be relevant with the presence of LA thrombus (P = 0.75).
Conclusion: Left atrial thrombus was present in 38% patients with severe mitral stenosis associated with atrial fibrillation. Larger left atrial diameter is a stronger predictor of presence of LA thrombus (JPMA 60:439; 2010).
Introduction
The incidence of Mitral Stenosis (MS) has decreased in developed countries due to impressive alleviation of rheumatic fever. However, in our part of the world it is one of the major health problems and a great challenge for the health care professionals.1-3
In patients with pure MS, left ventricle is usually normal but the left atrium is enlarged and hypertrophied as a result of increased LA pressure. Moreover, patients with severe symptomatic MS, 50% or more have chronic AF.4 Both LA enlargement and AF may alter the course of disease by providing the potential source of mural thrombi (LA clot) and the risk of systemic embolism.5,6 Apart from cerebral embolization these emboli may result in occlusion of arteries of the extremities, occlusion of the aortic bifurcation and visceral or myocardial infarction.4
Due to these serious implications of LA thrombus, it is mandatory to search the LA in every patient of MS for any evidence of thrombus especially if it is presenting with AF.4 Echocardiography is the best noninvasive method for detecting the LA thrombus. However there are well-recognized limitations in detecting LA thrombus by 2-D transthoracic echocardiography (TTE) especially those in the LA appendage.7
Transesophageal echocardiography (TEE) has been shown to overcome this problem and has proved to be highly sensitive for detecting LA thrombi.8-11 Once a thrombus is detected in LA the treatment plan, strategies, surgical and interventional techniques are greatly altered.9
Despite the fact that LA thrombus is very common in association with severe MS and atrial fibrillation; the prevalence in our vulnerable population was not known due to lack of local studies and data. This study provides us the data by which we can quantitate the proportion of patients having LA thrombus among this high-risk group i.e. patients with MS and atrial fibrillation. Moreover, this data will also help us to realize the magnitude of the problem, making right health strategies and decision about the issues of anticoagulation in different settings of severe MS.
Patients and Methods
This cross sectional descriptive study was conducted in Echo department of National Institute of Cardio Vascular Diseases (NICVD) Karachi from October 1, 2007 to March 17, 2008.
Patients with clinical findings of MS were screened. Those patients with severe MS and AF were selected for this study. A written informed consent was obtained, a previously designed study proforma/questionnaire were filled and information regarding personal details, history, clinical examination, findings of ECG and echocardiogram was documented.
All the patients having age of 18 years or above, who were found to have absent or fibrillatory P waves with varying R-R intervals on surface ECG and their 2-D echo examination showing mitral valve area of 1.0 cm² , were included in this study. Parasternal long- and short-axis views, the apical four-chamber view and apical long-axis view were obtained to detect LA thrombus. A LA mass was suspected whenever a conglomeration of echo densities were seen in LA cavity that persisted despite multiple alterations in gain and reject settings.
A LA thrombus was suspected when the mass of densities showed a relatively well circumscribed, defined border with some motion throughout the cardiac cycle, demonstrable in two or more echocardiographic views taken in different anatomic planes, showing the constant and reproducible position of the echo mass in the LA cavity and a surface attachment to the LA wall in at least one echocardiographic projection with an acoustic density of echo mass different from that of adjoining cardiac structures. TEE was performed whenever the nature of mass was controversial or thrombus could not be detected with conventional 2-D transthoracic echocardiography.
Patients with significant (moderate or severe) mitral insufficiency or any other significant valvular or congenital heart disease besides severe MS, patients with Left ventricular dysfunction, Hypertensive heart disease, Thyrotoxicosis, Chronic obstructive airway disease (COAD) were excluded from the study.
The data was analyzed by SPSS version 10. The measurable (quantitative) variables such as age, mitral valve area etc. was presented by mean + S.D value and compared, where required, by student\'s t-test. The various proportions of qualitative data were also presented by 95% confidence interval. The difference in proportions was compared by chi-square test of proportion, wherever needed.
Results
Out of 157 patients screened, 100 patients fulfilled all criteria and were included in the study. There were 52 male and 48 female patients with the mean age of 39.20 ± 11.41 years. All patients presented with history of palpitation and shortness of breath on exertion (NYHA class II - III) and 68 patients gave the history of orthopnoea and paroxysmal nocturnal dyspnoea while 12 patients had history of thromboembolic event in the past.
Mean mitral valve area of 100 patients was 0.82 ± 0.14 cm2, while mean values of pressure gradient across mitral valve, pressure half time and LA dimension were 24.04 ± 6.38 mmHg, 269.62 ± 43.83 ms, and 58.58 ± 13.50 mm respectively.
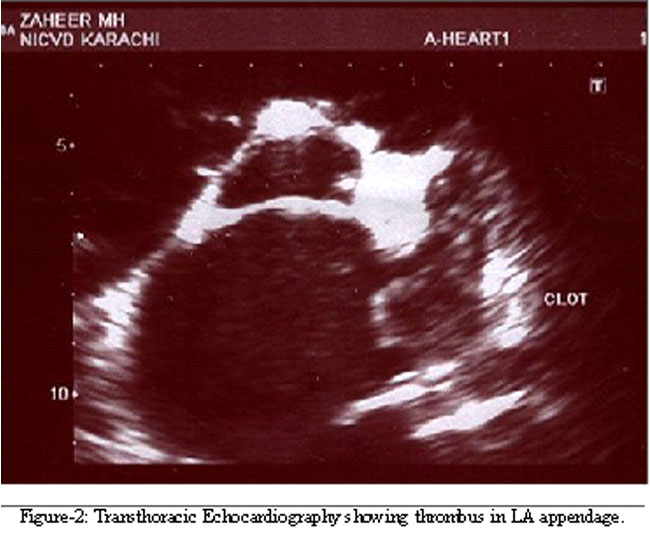
All the patients underwent transthoracic echocardiography that revealed thrombi in LA appendage in 18 patients and thrombi in LA body in 6 patients. Remaining 76 patients underwent TEE that revealed thrombi in LA appendage in 14 patients. No thrombus was detected in LA body with the help of TEE. LA spontaneous echo contrast (LASEC) was found in 54 patients. Out of these 54 patients; 28 had LA thrombi while 26 were free of any thrombus.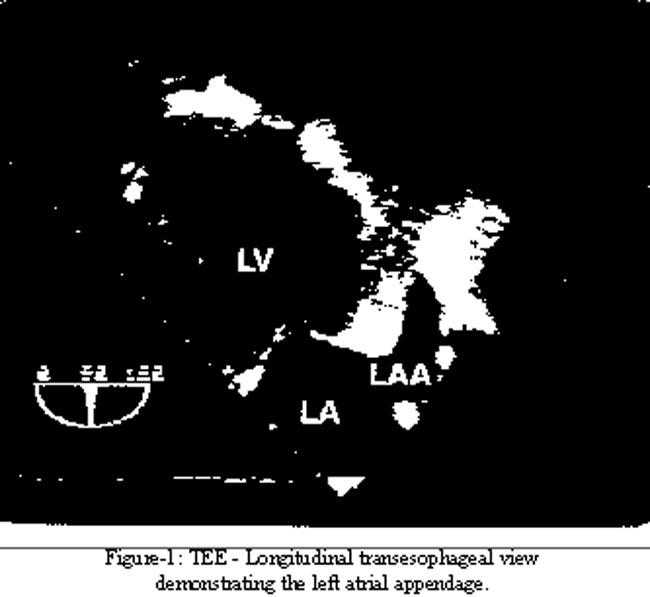
The comparison of mean values among age, mitral valve area, pressure gradient across mitral valve and pressure half time, when done by student\'s t - test, showed non significant differences among patients with presence or absence of LA thrombus. The only variable that was found to be relevant was LA dimension (63.53 ± 15.79 mm versus 55.55 ± 10.94 mm, P = 0.004) (Table).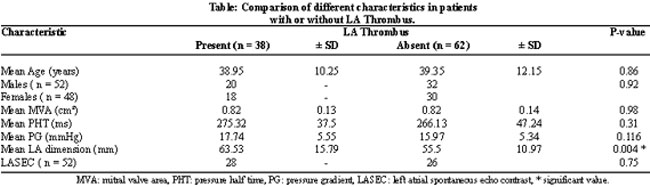
Discussion
Rheumatic mitral stenosis with atrial fibrillation is a common clinical problem in Pakistan.1-3 It is a potential source of thrombus formation and associated with a very high risk of embolic cerebro-vascular accidents, which is reported to be as much as seventeen times greater than in unaffected controls.12
TEE is well established as the gold standard for detecting thrombi in the left atrium and the LA appendage. The sensitivity and the specificity of TEE are reported to be 100% and 99%, respectively.13 Though it is known that thrombi are common in patients with MS and AF, until recently only small studies have documented the exact frequency of occurrence of these thrombi. In a small group of 50 patients with MS and AF, Hwang et al.8 observed an LA thrombus in 28 patients (56%) by TEE. In another small study of 22 patients with MS and AF, Karatasakis et al.14 observed an LA thrombus in 12 patients (54%).
However, recently Srimannarayana J et al.15 studied 490 patients with severe MS and AF and observed LA thrombi in 163 (33.5%) patients. We found LA thrombus in 38% patients in a group of 100 consecutive patients. Considering the size of the study group though the number of patients in our study group is little less for the prevalence of LA thrombi in patients with severe MS and AF but the results were comparable. Thus, it can be stated that 1 out of every 3 patients with severe MS and AF will have an LA thrombus.
Another important finding emerged in our study is almost the equivalent male to female ratio of disease (Male: Female = 1: 1.08). Whereas it is a known fact that the mitral stenosis affected women more than the men but majority of these studies are western. In our society the reason behind male predominance seems to be related to socioeconomic bias as reported by Rehman S16 in his study.
Our study showed that LA size is relevant with the presence of LA thrombus (63.53 ± 15.79 mm versus 55.55 ± 10.94 mm, P = 0.004). This means that larger the atrial size greater the chances of presence of LA thrombus in patients with severe MS and AF. While describing clinical risk factors for thrombus formation among patients with severe MS Goswami et al16 documented the same finding. Apart from LA diameter he found that longer duration of symptoms and more frequent atrial fibrillation with spontaneous echo contrast were independent risk factors for LA thrombus formation. Surprisingly we did not find the LASEC to be relevant with the presence of LA thrombus. We found it in 54% of patients, out of them 28 had LA thrombi while 26 were free of any thrombus (P = 0.75). Goswami et al19 observed LASEC in 53.5% of cases in their study but they enrolled all the patients with severe MS irrespective of having AF. This may be the reason of difference in our finding. However, at least it can be said that larger LA diameter is an alarming sign and one has to carefully look for LA thrombus in these patients.
In our study we performed TEE in 76% patients in whom LA thrombus was not detected by TTE. In remaining 24 % patients LA thrombus was detected by TTE. Out of these 24 patients we were able to detect the thrombi in 18 patients even in LA appendage. While with TEE thrombi were detected in LA appendage in 14 of 76 patients, which would have been missed if TEE was not performed. More interestingly, with TTE thrombi in LA appendage were detected in 18% patients. This finding reflects the ability of TTE to visualize the clot in LA appendage. Goswami18 addressed the same issue another study and concluded that sensitivity of TTE in visualizing the clot in LA appendage in south east Asian patients is not so bad as reported in west. In our part of the world patients are generally younger, have lesser body weight and thinner chest walls resulting in better transthoracic echogenecity. Due to these factors we did not perform TEE in those patients in whom LA thrombi were already detected with TTE. It would be unethical if TEE was performed unnecessarily, as it is comparatively an invasive procedure. Moreover, this deficiency did not effect our objective to evaluate the sensitivity and specificity of TTE in detecting LA clots.
Study Limitations:
According to selection criteria, we excluded the patients with severe MS and AF in whom left ventricular dysfunction was also present. Therefore the statistics of this particular group is not known. TEE was also not performed in patients in whom LA thrombus had been detected by TTE. Although possibility of LA myxoma in patients with severe MS is extremely rare but there are some case reports of having LA myxoma in patients with MS.19-22 Differentiating LA thrombus from myxoma is a challenge and it is difficult merely on TTE and hence TEE should be opted.
The present study was conducted at National Institute of Cardiovascular Diseases, one of the largest tertiary care centers of densely populated city of Karachi. This center receives patients from almost every part of the city and hence results of our study reflect the diseased status of Karachi only. To learn about the exact prevalence of the disease, a multi-center study should be conducted.
Conclusion
The proportion of patients with LA thrombi in patients suffering from severe MS and AF observed in this study was 38% (28.8 - 47.7; 95% CI). Therefore it can be stated that more than one third of the patients with severe rheumatic MS and AF will have LA thrombi. Larger LA diameter was observed statistically significant as far as the presence of LA thrombus was concerned. Therefore, larger the LA size in patients with severe MS and AF greater the frequency of having LA thrombus is expected. Hence, it is prudent to anticoagulate this high-risk group of patients to prevent them from serious implications of systemic thromboembolism.
References
1.Ullah K, Ahmed SA, Badsha S, Khan A, Kiani MR. Rheumatic Heart disease - A study of surgically excised cardiac valves and biopsies. J Coll Physicians Surg Pak 2002; 12: 542-5.
2.Chagani H, Aziz KU. Clinical Profile of Acute Rheumatic Fever in Pakistan - A prospective study. Pak Paed Cardiol J 2001; 3: 10-9.
3.Khan RF, Imtiaz Y, Ali H, Khan MU, Ali M, Riaz N, et al. Natural History and Relative Distribution of Different Valvular Heart Diseases in Mayo Hospital, Lahore. Ann King Edward Med Coll 2002; 8: 90-1.
4.Rahimtoola SH, Enriquez-Sarano M, Scheff HV, Frye RL. Mitral valve disease.In: Fuster V, Alexander RW, Rourke RA. Hurst\'s The Heart. 10th Ed. New York: McGraw-Hill 2001; pp 1697-727.
5.Tahir MZ, Ahmed ME. Cerebral embolism in chronic atrial fibrillation. Pak J Cardiol 1996; 7: 65-7.
6.Boonyasirinant T, Phankinthongkum R, Komoltri C. Clinical and echocardiographic parameters and score for the left atrial thrombus formation prediction in the patients with mitral stenosis. J Med Assoc Thai 2007; 90 Suppl 2: 9-18.
7.Shrestha NK, Moreno FL, Narciso FV, Torres L, Calleja HB. Two - dimensional echocardiography diagnosis of left atrial thrombus in rheumatic heart disease. A clinicopathologic study. Circulation 1983; 67: 341-7.
8.Hwang JJ, Chen JJ, Lin SC, Tseng YZ, Kuan P, Lien WP, et al. Diagnostic accuracy of transesophageal echocardiography for detecting left atrial thrombi in patients with rheumatic heart disease having undergone mitral valve operations. Am J Cardiol 1993; 72: 677-81.
9.Aschenberg W, Schluter M, Kremer P, Schroder E, Siglow V, Bleifeld W. Transesophageal two - dimensional echocardiography for the detection of left atrial appendage thrombus. J Am Coll Cardiol 1986; 7: 163-6.
10.Zaman KS, Sultan A. The comparative value of transesophageal and transthoracic echocardiography in detection of clot in left atrium. Pak Heart J 1994; 27: 25-8.
11.Messika ZD, Lung B, Brochet E, Himbert D, Serfaty JM, Laissy JP, et al. Evaluation of mitral stenosis in 2008. Arch Cardiovasc Dis 2008; 101: 653- 63.
12.Greenblatt DJ, Sellers EM, Shader RI. Drug therapy: drug disposition in old age. N Engl J Med 1982; 306: 1081-8.
13.Manning WJ, Weintraub RM, Waksmonski CA, Haering JM, Rooney PS, Maslow AD, et al. Accuracy of transesophageal echocardiography for identifying left atrial thrombi. A prospective, intra-operative study. Ann Intern Med 1995; 123: 817-22.
14.Karatasakis GT, Gotsis AC, Cokkinos DV. Influence of mitral regurgitation on left atrial thrombus and spontaneous echocardiographic contrast in patients with rheumatic mitral valve disease. Am J Cardiol 1995; 76: 279-81.
15.Srimannarayana J, Varma RS, Satheesh S, Anilkumar R, Balachander J. Prevalence of left atrial thrombus in rheumatic mitral stenosis with atrial fibrillation and its response to anticoagulation: a transesophageal echocardiographic study. Indian Heart J 2003; 55: 358-61.
16.Rehman S, Shabbier G, Shahid M. Clinical presentation of Infective Endocarditis. J Postgrad Med Inst 2002; 16: 55-63.
17.Goswami KC, Yadav R, Rao MB, Bahl VK, Talwar KK, Manchanda SC. Clinical and echocardiographic predictors of left atrial clot and spontaneous echo contrast in patients with severe rheumatic mitral stenosis:a prospective study in 200 patients by transesophageal echocardiography. Int J Cardiol 2000; 73: 273-9.
18.Goswami KC, Narang R, Bahl VK, Talwar KK, Manchanda SC. Comparative evaluation of transthoracic and transesophageal echocardiography in detection of left atrial thrombus before percutaneous transvenous mitral commissurotomy. Do all patients need tranesophageal examination? Int J Cardiol 1997; 62: 237-49.
19.Sim EK, Lim YT, Ng WL, Goh JJ, Reebye S. Co-existing left attrial thrombus and myxoma in mitral stenosis-a diagnostic challenge. Singapore Med J 1999; 40: 46-7.
20.Mahdhaoui A, Bouraoui H, Amine MM, Mokni M, Besma T, Hajri SE, et al. The transesophageal echocardiographic diagnosis of left atrial myxoma simulating a left atrial thrombus in the setting of mitral stenosis. Echocardiography 2004; 21: 333-6.
21.Khania M, Hekmat M. A patient with rheumatic mitral stenosis and an atrial myxoma. Eur J Echocardiogr 2003; 4: 229-31.
22.Stoddard MF, Liddell NE, Korfhage L, Arce J, Kupersmith J. The transesophageal echocardiographic diagnosis of left atrial myxoma simulating a left atrial thrombus in the setting of mitral stenosis. Clin Cardiol 1992; 15: 379-82.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: