
Hamidollah Bahador ( Faculty of Medicine, Iran University of Medical Sciences, Tehran, Iran. )
Abdolreza Pazooki ( Surgery, Iran University of Medical Sciences, Tehran, Iran. )
Ali Kabir ( Nikan Health Researchers Institute, Medical Education Department, Iran University of Medical Sciences, Tehran, Iran. )
June 2010, Volume 60, Issue 6
Original Article
Abstract
Objective: To examine the satisfaction and perception of participants with the current CME programme in Iran and eventually to re-design the programme accordingly.
Methods: In this descriptive cross-sectional study the attitude of participants in 28 CME programmes of Iran University, Iran, implemented between 2007 and 2009 were evaluated. A questionnaire was prepared (reliability coefficient of Cronbach\'s alpha = 0.97) consisting of seven main questions (Likert scale) related to attitude of participants about the quality of programme\'s content, lecturer teaching skills and participant`s learning and satisfaction; three open questions about weaknesses and strengths of the programmes and their recommendations about it; gender, type and duration of different programme. Our participants (physicians, nurses, midwives, health care providers, dentists, clinical laboratorists and nutritionist) completed the questionnaire at the end of their CME programmes.
Results: According to total score of the questions > 28, only 47.7% believed that the CME programme was effective. Workshops were more effective than seminar sessions (61.5% vs 30.1%, p<0.001). Total score of participant`s attitude was significantly higher in male in comparison with female (24.6±0.48 vs 22.9±0.54, p=0.02) and also significantly higher for workshops than seminars (28.2±0.21 vs 24.3±0.31, p<0.001). Effective programmes (total score > 28) had significantly lower duration (18.1±0.39 vs 19.1±0.34 hours, p=0.044).
Conclusion: While short course workshops are preferred in our community, effective, dynamic, and interactive educational methods in CME programme should be considered in this area as well (JPMA 60:435; 2010).
Introduction
Lifelong learning has been identified as an element of professionalism in medicine.1 Continuing Medical Education (CME) has an important role for professionalism in practitioners.
CME organizers should tailor appropriate programmes to meet the needs of participants in order to improve and increase the efficacy of their programmes. Audit and feedback of CME concerning behavioural changes in CME audiences is essential to assess the CME programme effectiveness. The effectiveness of CME should be objectively evaluated by assessing their impact on participant\'s learning and performance.2-5
In the Islamic Republic of Iran, continuing medical education strategy based on a special act of national parliament in 1973, the Iranian council of CME is responsible for supervision of the quality of graduate medical professionals in delivery of public health services.6
The general aim of present CME programmes in Iran illustrated through the following objectives: a- The physicians, nurses, midwives and other health care providers should be developed and their knowledge, skills and professional competence updated. b-The CME participants should be familiar with community health strategies, providing health services and priorities of public health problems. c-The prior accurate knowledge, exposure to effective health services and occupational standards of CME audiences must be reinforced.7 On the other hand, recertification of physicians, nurses and other health professionals should be a main component of CME.
In recent years, revision of the present medical education curriculum in Iran and other countries revealed that traditional methods of CME were not efficient in achieving the professional competence.8-10 In order to re-design CME programmes we carried out this study to examine the satisfaction and perception of participants with the current delivery of CME programmes in Iran.
Materials and Methods
In this descriptive, cross-sectional study we evaluated attitudes of participants in all 28 CME programmes of Iran University of Medical Sciences (IUMS) between December 2007 and July 2009. We prepared a primary questionnaire after a systematic review of the literature and expert panel discussions. Then we provided the face and content validity of the questionnaire by consulting experts in the field of medical education, designing questionnaire and KAP surveys. According to a pilot study on 56 cases, the reliability coefficient of Cronbach\'s alpha was 0.97. The final questionnaire consisted of seven main questions using a Likert scale related to attitude of participants about the quality of programme\'s content, lecturer teaching skills and participant`s learning and satisfaction; three open questions about weaknesses and strengths of the programmes and their recommendations about the CME programmes; and other variables such as gender, type of programmes (workshop or seminar) and duration of different programme. Positive attitudes in participant\'s feedback was assessed by open questions in the questionnaire as CME programme strengths and negative attitudes as weaknesses, respectively.
Our participants were physicians, nurses, midwives, health care providers, dentists, clinical laboratorists and nutritionists who completed the questionnaire at the end of their CME programmes. Our Liker scale had five grades from very high (score=5) to very low (score=1). Total score for each questionnaire was calculated by summation of all seven weighted (by their grade of Liker scale) main questions. In the present study, effectiveness was defined as a total score equal to or more than 28.
We used mean±SE (standard error), Chi-Square, t-test, Pearson\'s correlation coefficient and Cronbach`s alpha coefficient in our analysis using SPSS 16. In this study, the significant level was considered as 0.05 except for correlation test which was assumed as 0.01. The ethical committee of IUMS, Iran approved the proposal.
Results
Of 799 CME attendances, 366 (48.8%) participated in seminar and 433 (54.2%) in workshop and 50.4% were male. Duration of CME programmes was 18.8±0.2 hours (ranging from 8-40 hours). According to total score of the questions more than 28, only 47.7% believed that the CME programme was effective. Workshops were more effective than seminar sessions (61.5% vs 30.1%, p<0.001).
Total score of participant`s attitude was 26.5±0.19 (ranging from 7 to 35). It was significantly higher in males in comparison to females (24.6 ± 0.48 vs 22.9 ± 0.54, p=0.02) and also significantly higher for workshop than seminars (28.2±0.21 vs 24.3±0.31, p<0.001). Total scores of participant`s attitude was weakly correlated with duration of the programme (r=-0.13, p<0.001). Effective programmes (total score > 28) had significantly lower duration (18.1 ± 0.39 vs 19.1 ± 0.34 hours, p=0.044).
Because of clear briefing of the questionnaire`s content and CME audiences attitudes about their scores related to each question, we integrated very high (score=5) and high scores (score=4) as high grade, score=3 as the moderate grade and score=2 and score=1 as the low grade (Table 1).
The effectiveness rate of multiple types of programmes on participant\'s attitude was shown that the most attractive programme was "ostomy care management" in seminar format. In contrast, the seminar of "pharmacologic problems in clinical settings" had the lowest effectiveness rate (Table-2).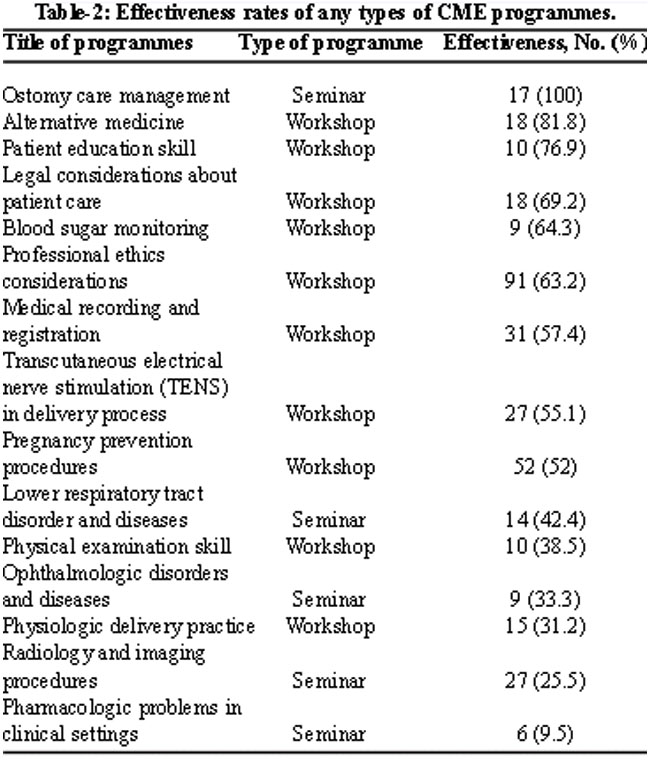
The highest priority of participant`s positive attitude about CME programmes was the updating their knowledge by application of programme`s content on the occupational setting and the lowest was dynamic and effective group discussion panel. Incorporation of high qualified lecturers in running of CME programme was the second positive priority (Table-3).
The weaknesses of CME programmes as the negative attitudes of participants were included in four distinct items (Table-3). The participant`s opinion about CME programmes designing, running and logistic were negative. These negative view points were also seen in CME director and instructor behaviours. It had highest percent value (63.3%). The lowest percent value was regarding CME credit in relation to expensiveness of administrative fee (2.6%).
Recommendations of CME participants were divided in two parts. One part was overall comments about the running process of programme. For example, increasing capacity and periodic repetition of programmes with reinforced proper public announcement of audiences had the highest percent value (45.7%). The other part illustrated recommended topics for CME programmes, in this part where the lowest priority was geriatric medicine with 0.3% value (Table-3).
Discussion
The CME system is highly specific part of the medical education setting. CME for physicians and other health personnel is an important component of recertification requirement. The challenge of assessing the effectiveness of CME system is formidable. This study, has evaluated the attitude of CME participants towards the traditional programmes which have three main objectives regarding different aspects of the Iranian Council of CME system. In our study, success rate of programmes to develop updated and to improve participant`s prior knowledge had the highest score. The relevance between programme content and participant`s occupational needs, and improvement in their professional competence were relatively high. In the other surveys, the explicit commitment of participants to lifelong learning and improving the professional behaviour change is a key factor for effectiveness and high quality of CME activities. These surveys show that the interventions about objectively assessment of physician performance and health care outcomes (at least 166 intervention) influences the physician performance (70%) and positive change in health care outcomes (48%).4
The widely used CME methods such as seminars do not have direct impacts on improving professional practice. In contrast, the workshop format has a significant capacity for instruction of dynamic and interactive CME programme sessions.11,12 In the present study, the satisfaction of CME participants correlated with shorter length of programmes. A Canadian systematic review also showed that behavioural change can accrue from a short-course intervention and that this was facilitated when CME participants committed to make behavioural changes. Similarly, other studies have emphasized the construction of short length block-directed lecture based programmes.13-16 This study also assessed effectiveness rate of participants` attitude about types of CME programmes. The "ostomy care management seminar" had the highest score. While the lowest score correlated with "pharmacologic problem seminar". These findings suggest that the participants` satisfaction, does not only depend on programme structure but other factors also may have an influence. However, one systematic review shows that using mixed interactive (workshop) and didactic (seminar) formats (64% agreed with the mixed method in comparison to 32% who did not) and focusing on outcomes may increase the effectiveness of CME meetings.17
Our study shows some crucial information from the participant\'s personal positive and negative ideas about CME programmes. CME programme evaluation is essential as feedback may improve CME quality.3 In our study, appropriate updated programme content presented by an experienced lecturer was among the CME programme\'s strengths. On the other hand, the dynamic and interactive discussion panels, had the lowest scores and were considered a weakness of these programmes. A survey in Germany suggested that interactive methods of lecturing may lead to sustainable knowledge and high degree of satisfaction; but unfortunately, few interactive CME courses are offered.18 Regarding participants\' negative attitude, ineffective programme designing had the highest score value as a weakness of CME programmes and few CME credit had the lowest score. These findings indicate the importance of CME programming, auditing and giving participant`s feedbacks and assessing their educational needs.6-10 This study shows that irregular provision of CME programmes, inappropriate educational facilities and imperfect content presentation were important participant`s negative attitude as CME weaknesses. These findings reinforce the necessity of continuing evaluation, revision and improvement in the CME system.
According to participant recommendations for improving CME, increasing the capacity of the CME programmes by greater participation of CME audiences and initiation of new virtual programmes with shorter presentation had high score values. Other comments of CME participants revealed that programme content linked to job related needs of participants and written material or software for self-directed learning had moderate score values. One study has shown that in 92% of conference and 64% of journal review session participants were satisfied, but rural physicians recommended that they were more likely to use interactive video, print-based self-study methods, software or online internet teaching methods, which encourage them to use self-directed CME.19
In present study, the second part of participant`s comments were related to CME programme topics. The "intensive care management practice" title had the highest score, while the "geriatric health problems" had the lowest. Many systematic reviews and an American geriatric society study have shown that many community-based health professions and physicians are not familiar with geriatric medical fields.20,21 In this study, researchers also encountered a major gap related to geriatric medicine, which should be considered particularly in view of increasing longevity in Iran.
Conclusion
It is recommended that the following points and comments be considered for further studies and future improvement in CME:
1- CME curriculum designing should be based on public health problems. 2- Planning CME programmes based on participants\' needs to enhance their promotion. 3- Use effective, dynamic, and interactive educational methods in CME programme. 4- Developing standards for comprehensive evaluation of CME effectiveness. 5- Revising the CME system that would be simplified for specific audiences, and 6- CME programmematic linkage are recommended between medical schools, scientific medical associations and community hospitals using multimedia and instructional techniques such as on-line CME, videoconferencing, and virtual educational self-directed learning.
Acknowledgment
We would like to express our special thanks to Dr Hamid Reza Baradaran for his encouraging comments on the final draft. All participants of this survey are also gratefully acknowledged.
References
1.Veloski JJ, Hojat M. Measuring specific elements of professionalism: Empathy, teamwork, and lifelong learning. . In: Stern DT, ed. Measuring Medical Professionalism. Oxford, UK: Oxford University Press; 2006, pp 117-45.
2.Marinopoulos SS, Dorman T, Ratanawongsa N, Wilson LM, Ashar BH, Magaziner JL, et al. Effectiveness of continuing medical education. Baltimore: The Johns Hopkins University, Center E-bP; 2007 Contract No.: Document Number|.
3.Jamtvedt G, Young JM, Kristofferson DT, O`Brein MA, AD O. Audit and feedback: effect on professional practice and health care outcomes. Cochrane Database Syst Rev 2006; 19: 259.
4.Davis D. Dose CME work? An analysis of the effect of educational activities on physician performance or health care outcomes. Int J psychiatry Med 1998; 28: 21-39.
5.Overeem K, Faber MJ, Arah OA, Elwyn G, Lombart KM, Wollersheim HC, et al. Doctor performance assessment in daily practice : dose it help doctors or not? A systematic review. Med Edu 2007; 41: 1039-49.
6.Mirzazadeh A, Hashemi H, Nasirpour H, Fotouhi A, Yazdani K, Tavakoli S, et al. Establishment of new evaluation and accreditation system for graduate medical education in Iran. J Med Educ 2004; 5: 69-73.
7.Hosseini J. Continuing medical education in Iran. Iran J Med Educ 2000; 1: 26-35.
8.Azizi F. Medical education in Iran: past, new and future new horizons in medical education in Iran J med Educ 2003; 4: 43-5.
9.Walton H. Global demands on medical education: the case of Iran. Iran J Med Educ 2007; 1: 34-6.
10.Shakurnia A, Elhampour H, Marashi T, SH HS. Concordance of length and contents of continuing medical education programmes with educational demands of practicing general physicians in Khuzestan province. Iran J Med Educ 2006; 7: 26-32.
11.Ghosh AK. Organizing an effective continuous medical education session. J Assoc Physicians India 2008; 56: 533-8.
12.Thomson MA, O\'Brien MA, Freemantle N, Oxman AD, Wolf F, Davis DA, et al. Continuing education meetings and workshops : effects on professional practice and health care outcomes. Ann Emerg Med 2009; 53: 685-7.
13.Davis D, Thomson MA, Oxman AD, Haynes RB. Evidence for effectiveness of continuing medical education: A review of 50 randomized controlled trials. JAMA 1992; 268: 1111-7.
14.Rodenhouser P, Markert RG. Influence of continuing medical education workshops on participant learning. J Contin Educ Health Prof 1989; 9: 69-76.
15.Yousefi M, Rabiei M. A comparative study on structured continuing medical education programmes with 25 and 5 credit points according to viewpoints of general physicians in Golestan province. Iran J Med Educ 2007; 7: 169-73.
16.Pilvar A, Salami M. Compare effectiveness of traditional and new method of education in formal continuing medical education programme. Iran J Med Educ 2002; 2: 45-6.
17.Davis DA, Thomson MA, Oxman AO, Haynes RB. Changing physician performance: A systematic review of the effect of continuing medical education strategies. JAMA 1995; 274: 700-5.
18.Kuhne-Eversman L, Eversman T, Fischer MR. Team and case-based learning to activate participants and enhance knowledge: an evaluation of seminars in Germany. J Cont Educ Health Prof 2008; 28: 165-71.
19.Mamary E, Charles P. Promoting self-directed learning for continuing medical education. Med Teach 2003; 25: 188-90.
20.Thomas DC, Johnston B, Dunn K SG, Brett B, Matzko M, Levine SA. Continuing medical education and continuing professional development, and knowledge transition: improving care of older patients by practicing physicians. J Am Geriat Soc 2006; 54: 1610-8.
21.Levine SA, Brett B, Robinson BE, Stratos GA, Lascher SM, Gronville L, et al. Practicing physician education in geriatrics: lessons learned from a train-to-trainer model. J AM Gerit Soc 2007; 55: 1281-6.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: