
Figen Barut ( Department of Pathology, Faculty of Medicine, Bulent Ecevit University (Former: Zonguldak Karaelmas Unviersity), Zonguldak, Turkey. )
Nilufer Onak Kandemir ( Department of Pathology, Faculty of Medicine, Bulent Ecevit University (Former: Zonguldak Karaelmas Unviersity), Zonguldak, Turkey. )
Banu Dogan Gun ( Department of Pathology, Faculty of Medicine, Bulent Ecevit University (Former: Zonguldak Karaelmas Unviersity), Zonguldak, Turkey. )
Sukru Oguz Ozdamar ( Department of Pathology, Faculty of Medicine, Bulent Ecevit University (Former: Zonguldak Karaelmas Unviersity), Zonguldak, Turkey. )
July 2016, Volume 66, Issue 7
Case Reports
Abstract
T-cell/histiocyte-rich large B-cell lymphoma is an unusually encountered lymphoid neoplasm of stomach with aggressive course, and is an uncommon morphologic variant of diffuse large B-cell lymphoma. An ulcerated mass, 7x5x1 cm in size was observed within the gastrectomy specimen of a 76-year-old female patient. In cross sections, besides mature lymphoid cells displaying T-cell phenotype, a neoplastic formation composed of large, pleomorphic atypical lymphoid cells with, prominent nucleoli, vesicular nuclei and abundant eosinophilic cytoplasm displaying B-cell phenotype were observed. Meanwhile, histiocyte-like mononuclear cells and Reed-Sternberg-like multinuclear cells expressing CD68 and Mac387 were also observed. The diagnosis of the case was T cell/histiocyte-rich large B-cell lymphoma. This rarely encountered neoplasm should be kept in mind in the differential diagnosis of primary gastric lymphomas.
Keywords: T-cell/histiocyte-rich large B-cell lymphoma; diffuse large B-cell lymphoma; gastric malignancies.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common lymphoid malignancy among adults and constitutes approximately 40% of non-Hodgkin lymphomas.1-4 T-cell/histiocyte-rich large B-cell lymphoma (T/HRBCL) is a rare morphologic variant of DLBCL and represents 1-3% of DLBCL cases.1-6 T/HRBCL which has been first described by Ramsay et al. in 1988, is a rare lymphoid neoplasm still owing controversies about clinical and biological behaviour.2-4,6-8
Primary lymphomas with an increasing incidence day by day, constitute more than 8-10% of gastric malignancies, and B-cell variant is the most common encountered type. T/HRBCL displays quite rare extranodal involvement, and primary gastric T/HRBCL case has been first described by Toth and Elek in 1997.9 Like large B-cell lymphoma, T/HRBCL is a neoplasm of the stomach exhibiting an aggressive course, and it is accepted as a less common variant of DLBCL. Gastric T/HRBCL case that has been seldom reported up to date is presented in the light of the data outlined in the literature.
Case Report
A 76-year-old female patient, subjected to endoscopic biopsy in healthcare center due to a palpable mass with epigastric localization, 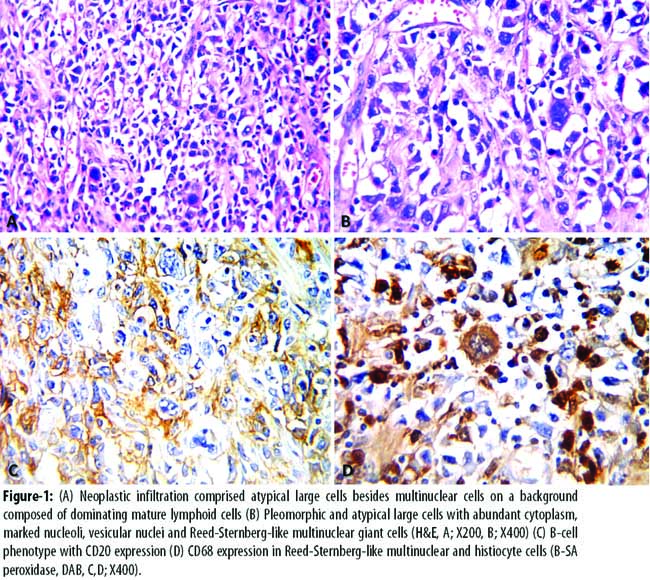
was diagnosed with \\\'malignant tumour\\\' and referred to the university hospital. After surgical intervention was performed,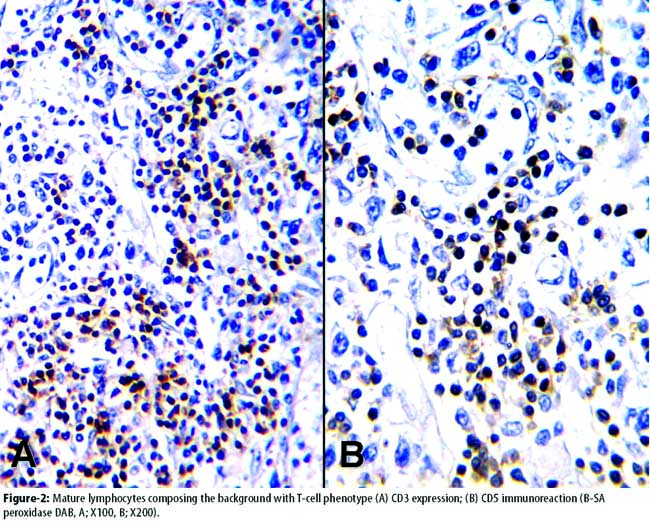
the resected specimen was examined and an ulcerated mass 7x5x1 cm in size was observed, which was infiltrating the serosa. The distances from the proximal and distal surgical margins were 1 cm and 2 cm, respectively. In cross sections of this ulcerated mass, a neoplastic formation was seen composed of the infiltration of histiocyte-like mononuclear cells and Reed-Sternberg-like multinuclear cells and mature lymphoid cells besides large pleomorphic atypical cells with abundant eosinophilic cytoplasm, prominent nucleoli and vesicular nuclei, as well (Figure-1A, 1B). The large cells with atypical lymphoid characteristics displayed a B-cell phenotype reaction with vimentin, LCA (CD45), CD20 (Figure 1C), and CD79a. Reed-Sternberg-like and histiocyte-like cells displayed CD68 (Figure 1D) and Mac387 expression; however, no reaction was determined with CD15 (LeuM1) and CD30 (Ki-1). T-cell phenotype reaction was observed with LCA (CD45), CD3, CD5 and CD45RO (UCHL-1) in the mature lymphoid cells (Figure-2A, 2B). No immunoreaction was observed in the tumour tissue with pankeratin, epithelial membrane antigen (EMA), Ber-Ep4, smooth muscle actin (SMA), desmin, CD117, CD34, bcl-2, CD10, and S100 protein.
The diagnosis was T cell/histiocyte-rich large B-cell lymphoma and three metastatic lymph nodes were determined. The patient was administered two cycles of chemotherapy. After the last chemotherapy cycle she did not attend the hospital again and was lost to followed-up.
Discussion
T/HRBCL is a recently defined, quite rare, B-cell lymphoproliferative disorder originating from germinal center cells with intermediate grade.1,2,5 Ramsay et al.7 first described it as a non-Hodgkin lymphoma characterized with scarce monoclonal B-cell groups distributed in a background of preponderant polyclonal T-lymphocytes, and proposed the term T/HRBCL. While diagnostic criteria have not been clearly defined, the presence of clonal B-cells comprising <10% or less of the total lymphoid cells is accepted as an adequate diagnostic criterion.1,2,5,8,9 Stromal reactive T-cells which are dominant in the neoplasm, are regarded as \\\'host immune response\\\' against neoplastic clone, and therefore with this feature, it resembles Hodgkin\\\'s disease.2,4,9
The most important problem for T/HRBCL in regard to histomorphological aspects is the difficulties on differential diagnosis. These lymphomas are frequently confused with peripheral T-cell lymphoma or Hodgkin\\\'s lymphoma accompanied with Reed-Sternberg-like cells.3,6,8-10 In regards of morphological features, it is very similar to Hodgkin\\\'s lymphomas, and neoplastic cells constitute the minor component of the lesion.10 Besides these, unlike Hodgkin\\\'s lymphoma, all the B-cells in T/HRBCL, have neoplastic features. Similar to the morphologic findings of the presented case, diffuse infiltration of neoplastic B-cells, with or without histiocyte increase, with a background almost completely comprising of reactive small T-cells, is observed in T/HRBCL.8-10 Small reactive B-cells are quite rarely seen.10 Cytologic features of both inflammatory background and the neoplastic component should be distinguished by immunohistochemical examination.3,9 With the use of immunohistochemical studies, it was demonstrated that, neoplastic cells were lymphocytes with B-cell phenotype (CD20, CD79a), meanwhile reactive small cells were lymphocytes with T-cell phenotype (CD3, CD5, CD45RO). No expression of CD15 and CD30 in Reed-Sternberg-like and histiocyte-like cells and the expression of CD68 and Mac387 in these cells helped us to distinguish T/HRBCL from Hodgkin\\\'s lymphoma.10 Without immunohistochemical studies, the distinction of primary gastric T/HRBCLs from other lymphomas, and also undifferentiated carcinomas, and soft tissue tumours, is very difficult.9
Most of the previously reported T/HRBCL cases were primary lymph node lymphomas with or without extranodal involvement. Recently, primary extranodal involvements were further defined related with the increase in number of cases due to widespread use of immunohistochemical method and molecular techniques.5,8,9 Extranodal involvements were seen in liver, bone, soft tissue, spleen, nasopharynx, brain, tongue, skin, uterus, and stomach.5 Mere primary extranodal involvement was reported quite rare. Aki et al. reported only one primary gastric T/HRBCL case, in a study conducted with a series of 21 cases.3
The stomach was the most frequently involved site for primary gastrointestinal lymphomas, frequencies of 44% to 75% were encountered in the literature. Gastric malignant lymphomas are generally classified as MALT (Mucosa-Associated Lymphoid Tissue) lymphoma and are frequently associated with Helicobacter pylori infection. Prognosis of gastric B-cell lymphomas are much better than those of nodal B-cell lymphomas, and survival depends on the histological grade, depth of invasion and lymph node metastasis. Although T/HRBCL differs from DLBCL according to clinical characteristics, it is recognized as a rare variant of DLBCL by WHO criteria, and same treatment regiment is applied.6,9
Conclusion
T/HRBCL is a rare neoplasm of stomach with an aggressive course and regarded as a different clinicopathologic entity originating from B-cells. An uncommon disease, T/HRBCL, should be kept in mind in differential diagnoses of primary gastric neoplasms.
References
1. Dominis M, Dzebro S, Gasparov S, Pesut A, Kusec R. Diffuse large B-cell lymphoma and its variants. Croat Med J 2002; 43: 535-40.
2. Abramson JS. T-cell/histiocyte-rich B-cell lymphoma: Biology, diagnosis, and management. Oncologist 2006; 11: 384-92.
3. Aki H, Tuzuner N, Ongoren S, Baslar Z, Soysal T, Ferhanoglu B, et al. T-cell/histiocyte-rich B-cell lymphoma: a clinicopathologic study of 21 cases and comparison with 43 cases of diffuse large B-cell lymphoma. Leuk Res 2004; 28: 229-36.
4. Achten R, Verhoef G, Vanuytsel L, De Wolf-Peeters C. T-cell/histiocyte-rich large B-cell lymphoma: A distinct clinicopathologic entity. J Clin Oncol 2002; 20: 1269-77.
5. Venizelos ID, Tatsiou ZA, Mandala E. Primary cutaneous T-cell-rich B-cell lymphoma: a case report and literature review. Acta Dermatoven APA 2008; 17: 177-81.
6. El Weshi A, Akhtar S, Mourad WA, Ajarim D, Abdelsalm M, Khafaga Y, et al. T-cell/histiocyte-rich B-cell lymphoma: Clinical presentation, management and prognostic factors: report on 61 patients and review of literature. Leuk Lymphoma 2007; 48: 1764-73.
7. Ramsay AD, Smith WJ, Isaacson PG. T-cell rich B-cell lymphoma. Am J Surg Pathol 1988; 12: 433-43.
8. Tajima K, Fukase N, Shiono T, Katagiri T, Mito S. An autopsied case of T-cell rich B-cell lymphoma with general involvement. Int Med 1995; 34: 243-6.
9. Tòth J, Elek G. Histiocytic and T-cell rich B-cell lymphoma (TCRBCL) of the stomach. Pathol Oncol Res 1997; 3: 219-23.
10.Zhao FX. Nodular lymphocyte-predominant Hodgkin lymphoma or T-cell/histiocyte rich large B-cell lymphoma: The problem in "Grey zone" lymphomas. Int J Clin Exp Pathol 2008; 1: 300-5.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: