
Abbas Ali Yousuf Tasneem ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
Hamza Aasim Yousuf ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
Nasir Hassan Luck ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
Zaigham Abbas ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
Sabiha Anis ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
Syed Mujahid Hassan ( Department of Hepatogastroenterology, Sindh Institute of Urology and Transplantation, Karachi, Pakistan. )
October 2015, Volume 65, Issue 10
Case Reports
Abstract
Autoimmune pancreatitis is characterised by diffuse enlargement of pancreas, narrowing of pancreatic duct, lymphoplasmacytic infiltrations and fibrosis. The disease is responsive to corticosteroid. We report the case of a 32-year-old male who presented with unilateral exophthalmos and obstructive jaundice secondary to pancreatic head mass and biliary tract stricture. Serum immunoglobulin G level was raised with a very high immunoglobulin G4 subclass. Ophthalmological imaging revealed unilateral thickening of extraocular muscles. The patient responded well to corticosteroid with resolution of biliary strictures, pancreatic head mass and exophthalmos.
Keywords: Autoimmune pancreatitis; IgG4-related systemic disease; Exophthalmos
Introduction
Autoimmune pancreatitis (AIP) is a form of chronic pancreatitis with autoimmune pathogenesis. The disease may be associated with involvement of other organs, including the biliary tract, gastrointestinal (GI) tract,retroperitoneum and kidneys.1 There are two categories of AIP: type 1 and type 2. Type 1 patients tend to be older, associated with high immunoglobulin G4 (IgG4) levels and have a high relapse rate, whereas patients with type 2 tend to be younger, are not associated with high IgG4 levels and do not experience relapse.2 The disease shows good response to steroid therapy with resolution of the pancreatic swelling, biliary strictures and extrapancreatic organ involvement.3 In some patients with AIP, usually only one or two organs are clinically involved whereas in other patients multiple organs may be involved. Here we report the rare case of an adult male with AIP along with biliary strictures and orbital involvement. To the best of our knowledge this is the first case report of AIP with extraocular muscles involvement from Pakistan.
Case Report
A 32-year-old male with history of asthma since childhood presented to our clinicin May 2012 with jaundice, epigastric pain andweight loss of 15kg over the preceding one year. General physical examination showed a protuberant left eye, which,according to the patient, was present for 12 years. Abdominal examination showed mild upper abdominal tenderness. He had sought prior medical consultation at another hospital where a computed tomography (CT) scan of abdomen was performed which revealed a dilated common bile duct (CBD), intra-hepatic duct (IHD)dilatation and a mass in the pancreatic head. Endoscopic retrograde cholangio-pancreatography (ERCP), performed about 10 months earlier, showed a distal CBD stricture for which a biliary stent was placed. The bilirubin levels had gradually decreased thereafter over a period of six months. A magnetic resonance cholangiopancreatography (MRCP) performed in our centre at the time of presentation, redemonstrated the pancreatic head mass measuring 2.2cm x 2.1cm, a distal CBD stricture and kinking of the distal pancreatic duct. Laboratory investigations showed a normal complete blood count (CBC) and deranged liver function tests (LFTs) with total bilirubinof 0.41 mg/dl, direct bilirubin 0.20mg/dl, alkaline phosphatase 774 U/L, gamma glutamyltranspeptidase 346 U/L, aspartate aminotransferase (AST) 56 U/L and alanine aminotransferase (ALT) 51U/L. ERCP was then performed for cholestatic LFTs. The previously placed plastic stent was removed, and the cholangiogramobtained showed an irregular CBD with two strictures, one in distal CBD and another in the proximal portion which extended into the right IHD. Two stents were placed, one each in the left and right ductal systems. Esophagogastroduodenoscopy and colonoscopy showed normal mucosa and histopathology revealed normal duodenal and colonic biopsies. Serological workup showed an elevated IgG value of 48.3G/L (reference range: 7.2-15.8 gm/L) with IgG4 level of 7.5 gm/L(reference range: 0.1-1.3gm/L). The level of CA 19-9 was normal i.e. 8.93 U/ml (routine: <33U/ml). The anti-nuclear antibody was weakly positive at a titer of 1:40, while the anti-smooth muscle antibody, anti-mitochondrial antibody and anti-liver kidney microsomal antibody were all negative. The viral serology, including hepatitis B surface antigen (HBsAg) and anti-hepatitis C antibodies (anti-HCV)were non-reactive. Liver biopsy showed minimally expanded portal tracts with lymphocytic infiltrate, fibrosis, occasional foci of lobulitis, mild focal cholestasis and no piecemeal necrosis. The modified histology activity index (HAI) stage was 2/6. The thyroid function tests were all normal but anti-thyroid peroxidase antibody level was found to be abnormally high i.e. 90.2 IU/ml (cut off <35 IU/ml). Thyroid scan showed normal uptake of radiocontrast. Anti-neutrophil cytoplasmic antibodies (ANCA), includingc-ANCA and p-ANCA, were negative. Magnetic resonance imaging (MRI) of the orbit showed thickening of all left-sided extra-ocular muscles, predominantly left lateral rectus and inferior rectus muscles with mild retro-orbital inflammatory changes and mild proptosis, consistent with orbital inflammatory pseudotumour (Figure-1).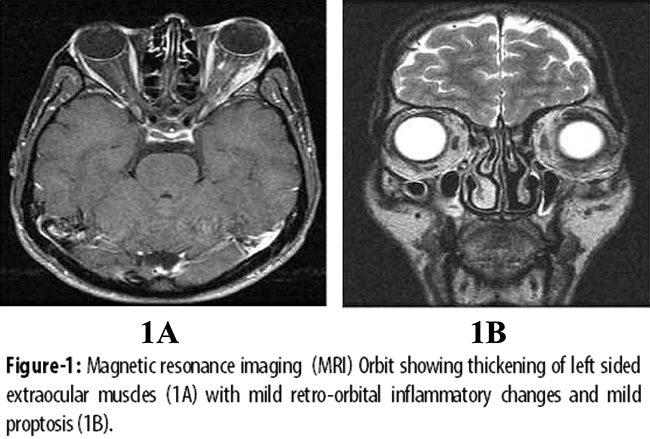
These investigations ruled out any hepatobiliary malignancy and strongly suggested the diagnosis of AIP type 1 with pancreatobiliary and orbital involvement.
Management was started subsequently with prednisone at a dose of 1 mg/kg/day, azathioprine 50 mg/day and ursodeoxycholic acid 250 mg thrice a day. Follow-up after 6 weeks showed improved LFTs. ERCP showed remarkable resolution of the strictures that were previously seen in the biliary tree (Figure-2).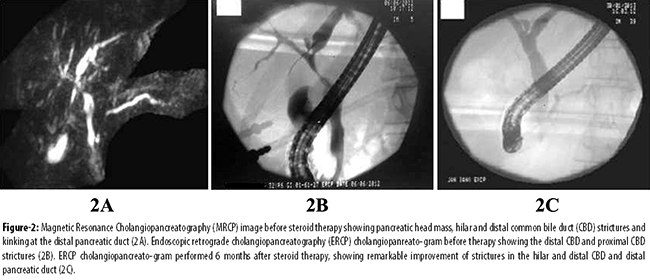
Repeat ultrasound abdomen showed resolution of pancreatic head mass. The proptosisof left eye also showed significant improvement (Figure-3).
Discussion
AIP associated with elevated IgG4 levels is a systemic disease that may involve different organs of the body. When coming across diseases with multi-organ involvement, AIP should be considered an important constituent of differential diagnosis because it can include diverse entities like pancreatitis, cholangitis, nephropathy, pericarditis and pseudotumors of the orbit. Further studies may reveal the growing list of organs that this disease may affect. The diagnosis of AIP is aided by the Mayo Clinic HISORT criteria which comprisesfive cardinal features; Histology, Imaging, Serology, Other organ involvement and Response to steroid Therapy.3 Patients with AIPshow a remarkable response to corticosteroid therapy with a resolution of jaundice and mass lesions of affected organs. The typical steroid dose is prednisone 30-40 mg per day for four weeks, followed by slow tapering by 5mg per week.4 Recurrence is seen in up to 40% of patients and these patients may be retreated with steroids and immunosuppressants.5
Our patient was diagnosed as AIP type I on the basis of clinical features, including obstructive jaundice, abdominal pain and unilateral exophthalmos; imaging findings of pancreatic mass, biliary strictures and orbital pseudotumour. Serological findings of high serum IgG and IgG4 levels, and a remarkable response to steroid therapy evidenced by resolution of pancreatic mass, biliary strictures and exophthalmos supported the diagnosis. However, our patient did require ERCP and biliary stenting for cholangitis that developed during the course of illness. The prevalence of AIP is seen globally as indicated by several case reportswith different organ involvements. A case with AIP together with inflammatory pseudotumors of the kidney and lung has been reported in Japan.6 The diagnosis was made on the histological, serological markers and effective response to steroids. An American case report showed gastric involvement in a patient with AIP.7 Here, the patient presented with abdominal pain and weight-loss with abdominal imaging showing pancreatic and stomach wall thickening and gastric biopsy showing extensive IgG4 associated sclerotic disease. In another British case report, pericardial involvement was demonstrated in a case of AIP.8 This British patient presented with cholestatic jaundice, pancreatic head mass and right heart failure secondary to pericardial thickening, the biopsy of which showed lymphocytes strongly staining with IgG4. In Japan, infraorbital nerve swelling was observed more frequently in AIP patients than in those without history of AIP.9 A study reported a case from Bristol, United Kingdom, of an orbital mass in a 5-year-old child which was due to IgG4 related orbital inflammation.10 This was the youngest reported case of IgG4 related disease. In our case, the patient had extra-ocular muscles involvement along with inflammatory pseudotumor in the orbit that caused exophthalmos. The patient\'s thyroid profile was normal, although the serum anti-thyroid peroxidase antibody level was high.
Conclusion
Treating the patient with immunosuppressants produced a good response. Histological analysis of pancreas could not be done as the patient was reluctant to undergo any invasive radiological or surgical diagnostic intervention.
Acknowledgement
We are grateful to the Sindh Institute of Urology and Transplantation (SIUT) for allowing us to conduct all the tests.
References
1. Takahashi N, Kawashima A, Gletcher JG, Chari ST. Renal involvement in patients with autoimmune pancreatitis: CT and MR imaging findings. Radiology 2007; 242: 791-801
2. Sah RP, Chari ST, Pannala R. Differences in clinical profile and relapse rate of type 1 versus type 2 autoimmune pancreatitis. Gastroenterology 2010; 139: 140-8.
3. Chari ST. Diagnosis of autoimmune pancreatitis using its five clinical features: introducing the Mayo Clinic\'s HISORt criteria. Gastroenterology 2007; 42: 39-41.
4. Efeovbokhan N, Makol A, Cuison RV, Minter RM, Kotaru VP, Conley BA, et al. An unusual case of autoimmune pancreatitis presenting as pancreatic mass and obstructive jaundice: a case report and review of the literature. J Med Case Rep 2011; 5: 253.
5. Frulloni L, Lunardi C, Simone R, Dolcino M, Scattolini C, Falconi M, et al. Identification of a novel antibody associated with autoimmune pancreatitis. N Engl J Med 2009; 361: 2135-42.
6. Nishikawa G, Nakamura K, Yamada Y, Yoshizawa T, Kato Y, Katsuda R, et al. Inflammatory pseudotumors of the kidney and the lung presenting as immunoglobulin G4 - related diseases: a case report. J Med Case Rep 2011; 5: 480
7. Baez JC, Hamilton MJ, Belizzi A, Koenrad JM. Gastric involvement in autoimmune pancreatitis: MDCT and histopathologic features. J Pancreas 2010; 11: 610-3.
8. Nayar M, Charnley R, Scott J. Autoimmune pancreatitis with multiorgan involvement. A case of pericardial involvement. J Pancreas 2009; 10; 539-42.
9. Watanabe T, FU jinaga Y, Kawakami S, HattaT, Hamano H, Kawa S, et al. Infraorbital nerve swelling associated with autoimmune pancreatitis. Jpn J Radiol 2011; 29: 194-201.
10. Kalapesi FB. IgG4 orbital inflammation in a 5-year-old child presenting as an orbital mass. Orbit 2013; 32:137-40.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: