
M.A. Arif ( National Institute of Child Health, Jinnah Postgraduate Medical Centre, Karachi. )
July 1982, Volume 32, Issue 7
Original Article
Abstract
Frequency of Rhesus and ABO blood groups was determined in 3012 mothers. The blood groups in order of frequency were B, O, A and AB. Only 6.2% mothers were rhesus negative.
ABO haemolytie disease of the newborn (HDN) accounted for 15.7% and Rh-HDN for 12.7% of 306 neonate admitted with Jaundice. No significant difference was found in two groups when levels of serum bilirubin, exchange transfusions and frequency of kernieterus were compared (JPMA32:165, 1982).
Introduction
Jaundice occurs in 60% of newborn infants (Behrman, 1975). Although it is physiological in majority of cases, but in some it may result in Kernicterus. Jaundice in neonates is commonly due to ADO and rhesus incompatibility. The frequency of these antigens differs in different races. While 15% of white population in USA is negative for rhesus antigen only 7% ofnegroes and 1 % of chinese are rhesus negative.
The frequency of ADO blood groups in women admitted in the obstetric ward and neonatal Jaundice due to blood group isoim munizatlon is reported in this study.
Material and Methods
In a prospective study from January 1977 to June 1980 rhesus and ADO blood groups of 3012 mothers admitted to the obstetric unit of J innah Postgraduate Medical Centre were determined.
Of 423 neonates admitted with Jaundice during this period 414 were included in this study, the remaining 9 either died or excluded soon after admission.
Detailed history of the paticnt, mother and siblings was obtained and a thoroñgh physical examination done. Blood counts, Hb, urine examination, chest radiographs, investigations a for haemolysis and blood group incompatibility were done in all patients.
Total and conjugated hilirubin was done by the modified method (Michaelsson et al, 1965) of Malloy and Evelyn (1937). S GET, screening test fbr G. 6P. P . deficiency and lumber puncture Were done when indicated.
Physiological jaundice was diagnosed by the following criteria:-
(1) Onset of jaundice later than 36 hours after birth.
(2) Peak total serum bilirubin not exceeding 12 mg% and indirect bilirubin not exceeding 10 mg%.
(3) Jaundice clinically disappearing by 10th day.
(4) Total biliruhin not increasing by more than 5 mg% per day.
ABO-HDN was diagnosed if infant and mother had different ADO blood groups and in addition 4 of the following were present:
(1) Jaundice appearing in the first 24 hours;
(2) Peak indirect hilirubin over 10 mg% in the first 48 hours
(3) ‘Total bilirubin level increasing by more than 5 mg% per day.
(4) Reticulocytosis of over 4%.
(5) Microspherocytosis.
(6) Positive direct combs test.
(7) Positive indirect Coombs test. RH-HDN was diagnosed when mother was Rh negative, baby Rh positive and the direct coomb’s test was positive. ‘T’ test was used to arrive at the significance between 2 averages. Significance of the difference between two proportions was tested by calculating their standard error (Hill, 1971).
Photo-therapy was given to all patients if the indirect bilirubin was more than 5 nig% on first day or over 10 mg% on any day. Exchange transfusion was done if serum indirect bilirubin level was approaching 20 mg% in the normal birth weight infants awl 15 mg% in the low birth weight infants.
Results
The blood groups of 3012 mothers are compared to those of American population (Sehaffer, 1965; Smith, 1966) in Table I.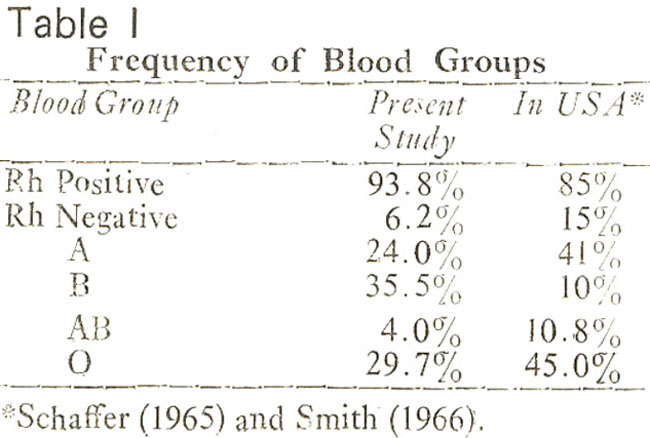
Of 414 jaundiced neonates studied 108 had physiological jaundice. These have not been included in further analysis. Out of 306 cases of Pathological jaundice, 48 (15.7%) had ABO-HDN and 39 (12.7%) had Rh-HDN. The mean weight of ABO-HDN group was 2666±466 grams and those with Rh-HDN was 2678±449 grams. The mean age on admission of ABO-HDN group was 4 36±2 8 days and that of Rh-HDN group was 51±5 7 days. The hacmoglobin and serum hiliruhin levels are shown in Table II.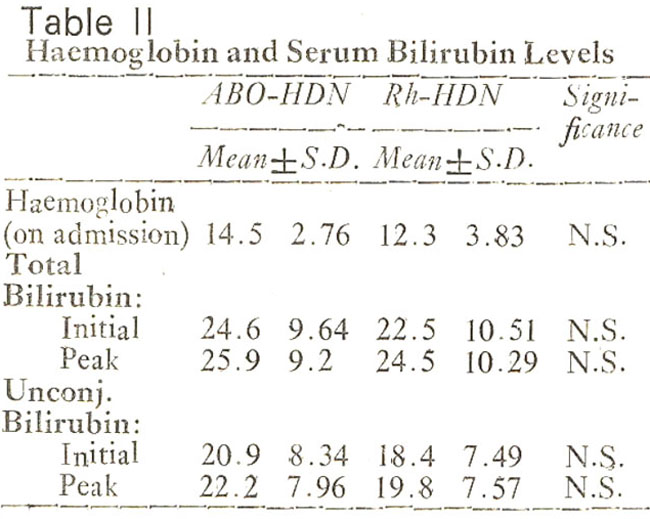
Twenty three infants (49.9%) of the ABO-HDN and'21 (53.8%) of the Rh-HDN were exchanged. Of all the 65 exchanges, 32 (49.2%) were done in ABO-HDN group while 33 (50.8%) were done in Rh-HDN groups. Kemicterus occurred in 7 (14.6%) infants of ABO-HDN and 6 (14.4.%) of Rh-HDN group.
Discussion
Only 6.2% of mothers in this study were rhesus negative as against 15% among" the white population of England (Keay and Morgan, 1974) and USA (Schaffer, 1965). It is also less than the 7% among American negroes but more than the 1% among Chinese (Behrman, 1975).
The cases of ABO-HDN out- numbered those of Rh-HDN. Similar findings have been reported from Vellore (Jadhav and Devanajan, 1972) and Chandigarh (Das et al., 1974) in India. In USA Rh-HDN is 3 times more frequent in white (Behrman, 1975; Kirkman, 1977).
Many European and American authors have remarked that ABO-HDN is a generally mild disease (Hutchison, 1967; Peevy and Wiseman, 1978; Clark, 1972). This is not our experience. We found no statistically significant difference in the peak bilirubin levels reached, the proportion of babies exchanged in each group and the proportion of babies developing kernicterus. it is possible that ABO-HDN is more severe in Pakistani children compared to the white children asis the case with black children in USA (Kirkman, 1977;Bucheretal., 1976). Thus considering both the frequency and the severity, ABO-HDN is more important for us in Pakistan than Rh-HDN.
Acknowledgement
The help of Dr. Khadija Shaukat and Dr. Shakoor A. Kazi is gratefully acknowledged.
References
1. Behrman, R.E. The fetus and the newborn infant, in Nelson\'s textbook of paediatrics. 10th ed. Philadelphia, Saunders, 1975, pp. 375-389.
2. Bucher, K.A., Patterson, A.M. Jr.,, R.C., Jones, C.A. and Kirkman, H.N. (1974) Racial difference in the incidence of ABO haemolytic disease. Am. J. Public Health, 66:854.
3. Clarke, C.A. (1972) Practical effects of blood group incompatibility between mother and foetus. Br. Med. J., 2:90.
4. Das, B.E., Bhakce, O.N. and Jolly, G.J. (1974) Neonatal hyperbilirubinaemia associated with gIucose-6-phosphatc dehydrogenase deficiency; a preliminary study. Indian Pediat., 11:645.
5. Hutchison, J.H. Practical paediatric problems, 2nd ed. London, Lloyd-Luke, 1967, p. 37.
6. Jadhav, M. and Devanajan, L.J. (1972) ABO haemolytic disease, and important cause of neonatal morbidity. Indian Pediatr., 9:246.
7. Craig, W.S. Care of the newly born infant. 5th ed. Edinburgh, Churchill-Livingstone, 1974, p. 324.
8. Khan, S.R. and Ahmad, S.A. Study of Jaundiced newborns in Nursery Proceedings. Fourth Biennial Conference of Pakistan Paediatric Association. Peshawar, 1978, pp. 79-82.
9. Kirkman, H.N. (1977) Further evidence for a racial difference in frequency of ABO haemolytic disease. J. Pediatr., 90-717.
10. Malloy, H.T. and Evelyn, K.A. (1937) The determination of bilirubin with the photoelectric ôalorimeter. J. Biol. Chem., 119:48l.
11. Michaelsson, M., Nosslin, B. and Sjolin, S. (1965) Plasma Bilirubin determination in the newborn infant. A methodological study with special reference to the influence of haemolysis. Pediatrics, 35:925.
12. Peevy, K.J. and Wiseman, H.J. (1978) ABO hemolytic disease of the newborn; evaluation of management and identification of racial and antigenic factors. Pediatrics, 61:475.
13. Schaffer, A.J. Diseases of the newborn, 2nd ed. Philadelphia, Saunders, 1965, p. 617.
14. Smith, C.H. Blood diseases of infancy and childhood. 2nd ed. Saint Louis, Mosby, 1966, pp. 126-139.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: