
Naghma-e-Rehan ( Public Health Research Unit, Ministry of Health, PMB 2018, Katsina, Kaduna State, Nigeria. )
July 1982, Volume 32, Issue 7
Original Article
Abstract
The prevalence and etiology of still-births were studied among 3858 Hausa infants born at Maternity Hospital, Katsina, Nigeria. The still-birth rate, 113/1060 births, was higher among grand multiparae and in women older than 35 or younger than 16 years. The lowest incidence of still-births was observed among secundiparae of 17 -19 years. Large age difference between spouses, advancing maternal age and increasing birth order were associated with higher still-birth rates. The most prominent etiolcgical factors were obstructed labour (2%), ante-partum hemorrhage (17%) and malpresentations (16.5%). The effect of certain social factors was also studied (JPMA 32:156, 1982).
Introduction
Two useful measures of the reproductive efficiency of any community are birth weight and perinatal mortality i.e., still-births and deaths within first seven days of life (W.H.O., 1961). There is a recognised variation in the value of these two parameters not only among different countries but also within various commumties of the same country depending on their socioeconomic and health-care levels. Nigeria is one example of such ethnic diversities. In previous papers we discussed birth weight (Rehan and Tafida, 1979), multiple pregnancy (Rehan and Tafida, 1980), and low birth weight (Rehan and Tafida, 1981) among Hausa population living in the northern part of this country and found consideraile dufferences from the population living in the hot and humid climate of the southern part of Nigeria. It was thus thought worthwhile to study the problem of still-birth among Hausa population, particularly in view of the fact that no such study has earlier been undertaken.
Apart from giving an insight into the obstetrical problems of a different country, the data are also relevant to Pakistan because many social problems like early marriages and large age differences among spouses particularly in rural areas, in-accessibility to basic medical facilities, lack of modern equipment and qualified profëssionals are common to both countries. The artele also gives a brief review of various causative factors and their modus operandii.
Methods and Material
From the records of all deliveries conducted at Maternity Hospital Katsina, between 1st january 1974 and 31st December 1977, the records of those infants were selected, whose both parents were Hausa. Due to lack of certain relevant data, the records for the months of January, February and june 1974 as well as those of November 1977, were excluded. From these records all cases of stillbirths were separated and studied in detail.Stillhiriths was defined as a fetus of more than 2 weeks gestation which, after complete expulsion or extraction from the mother, showed no sign of life such as beating of the heart, pulsation of umblical cord or definite movements of voluntary muscles (W.H.O., 1950).
The etiological factors were categorised according to the classification used by Grech (1967) and Ampofo (1971), whereas the age and parity groups used in Fig.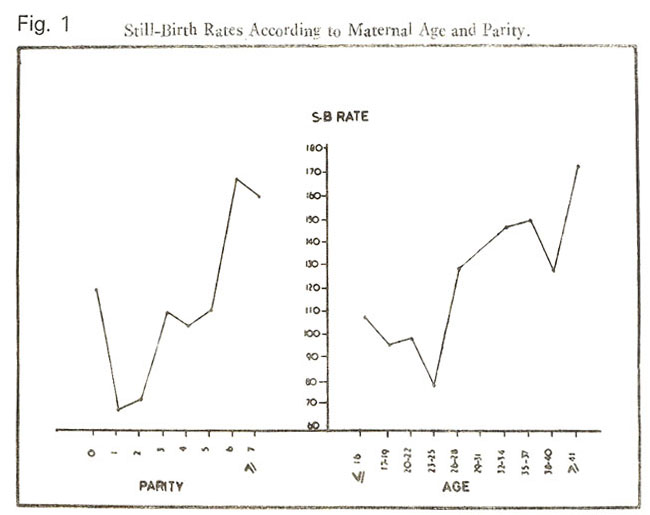
I were on the pattern of British perinatal Mortality Survey (1969) except the first two groups.
Description of. Area and Popi lation
Hausa is the name of the largest ethnic group of Nigeria, which is mainly resident in northern parts of the country. The detailed description of Hausas which appeared in our previous Papers (Rehan and Tafida, 1979, 1980; Rehan and Ahashiya, 1981) is summarised below.
Hausa is a linguistic, not an ethnic term, and refers to those whose mother tongue is the Hausa language (Hill, 1977). So far the Hausa were regarded as being people of the mixed stock. which resulted from the inter-marriages between Negroes and Hamitic people-a bramh of Medi- terranean race, named after Ham, the second son of Noah. However the recent research shows that this theory of racial origin is not correct (Smith, 1976; Adamu, 1978). It has now been proved that Hausas were autochthons in the areas, which is now called Hausaland (Adamu, 1978). The Hausa people are settled mainly between 10.5 and 13.5 degrees North and 4 to 10 degrees East, in a huge area in the north of Nigeria and the south of Niger Republic. The Hausaland Consists essentially of the basin of Sokoto river and its tributaries to the west and of a greater plateau to the east (Hill, 1977). Good farmers and skilled craftmen, the Hausas are known throughout Africa as remarkably clever traders.
In most parts of Hausaland, child marriage is the rule; both boys and girls are married at the age of 12 to 13 years in the large towns but at even younger ages in the villages (Madauci et al., 1968). Girls may be married before they reach puberty, so that some have their first menstrual period when they are already in their marital homes (Harrison, 1978). Consequently, the child hearing starts before their reproductive faculties are fully developed. Hausas are predominantly Muslims. Polygamy is widely practised and large family is a cherished desire. Only a minority of the women smoke, though the trends are changing with younger generations.
Katsina is situated in the extreme north of Nigeria and falls into the sudan zone of savanna. The climate is dry with a single peak wet season as compared to double wet season of the southern part of the country. The rainfall is about 260 mm and temperature ranges between 10°C and 40°C. Katsina is an ancient city and had been the maim centre of commerce and industry in Hausaland for over three hundred years from 15th century till 1807, when due to frequent political turmoils Katsina lost this position. The major trade routes into Hausaland led to Katsina and here the state of civilisation which has been called forth by contact with the Arabs seem to have reached its highest degree (Adamu, 1978). Katsina has also been a major centre of learning.
Results
During the study period, 3858 Hausa infants were born. Out of them 436 were still-born giving a still-birth rate (SBR) of 113/1000 total births.
Maternal Characteristics:
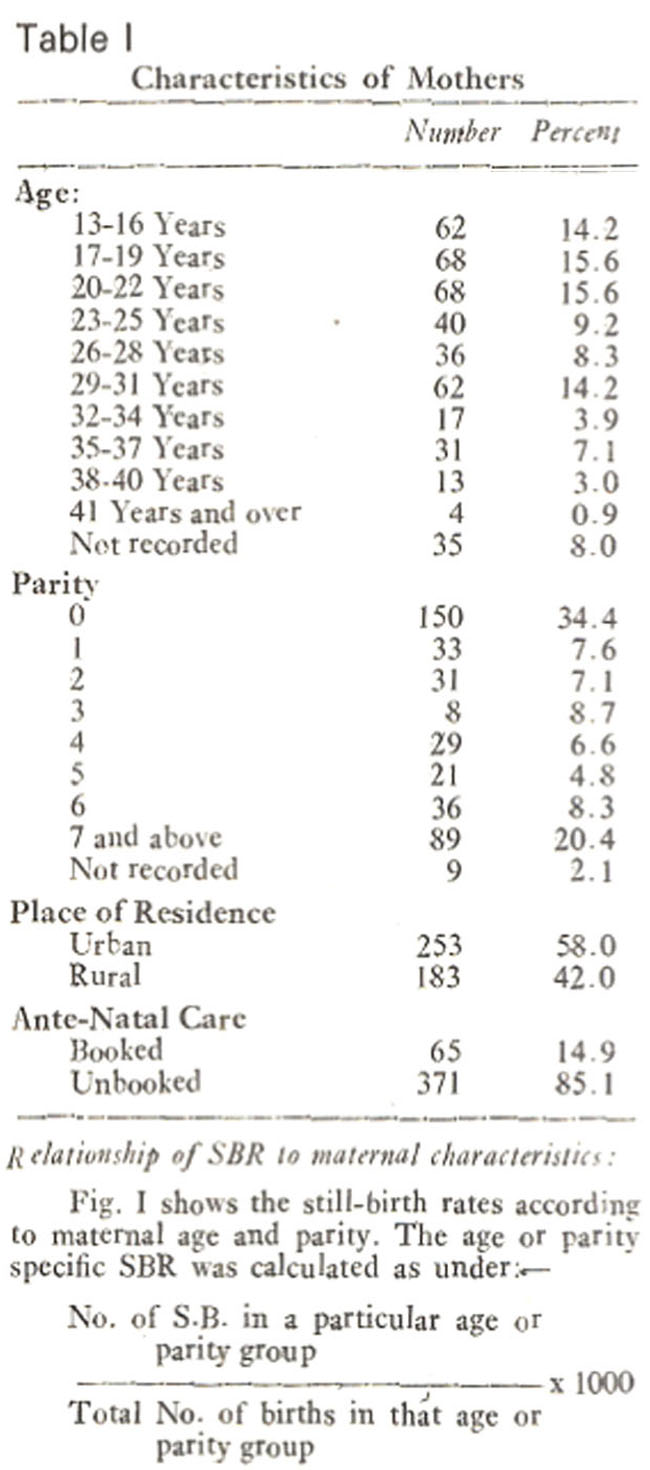
Table I summarises the characteristics of the mothers of these 436 still-born children. The maternal age ranged from 13 to 44 years (Mean+-S.D. being 24.2±6.9 years); 39.6% were 20 years or below. The parity ranged from 0 to 14. The primiparae formed the largest group (34.4%), while 20.4% were grand multipara i.e. parity 7 and above (Hughes, 1972; Greenhill, 1974).. Though the majority of these mothers were living in urban areas, yet only 14.9% had attended any ante-natal clinic. Based on the records of their husband’s occupations, these women can be considered as of low to middle socio-economic background.
There was a tendency in still-birth rate for an initial fall with the advancing maternal age and increasing birth order, so that the lowest still-birth rate was observed in 23-25 years age group and parity I. Then there was a sharp rise in the still-birth rate with increase both in maternal age and birth order. However when age-specific still-birth rates were calculated according to various parities (Fig. 2),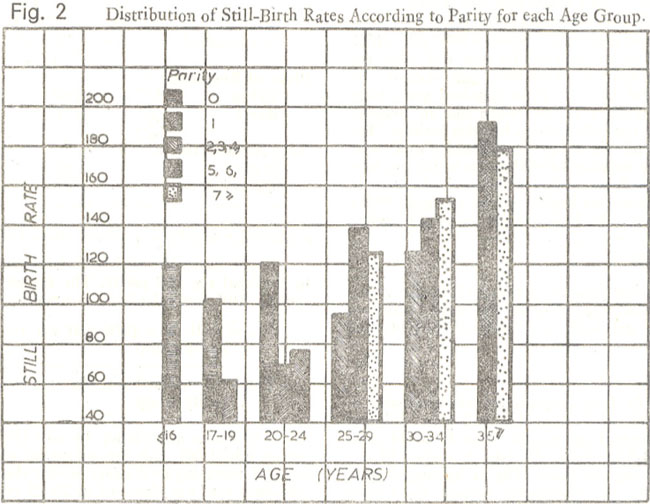
a sligh’ different picture emerged, showing the lowe incidence of still-birth rate among secundipat of 17-19 years. In Fig. 2 among some age grou certain parities have been omitted because the number of cases was too small to make any valid conclusions.
The still-birth rate was higher in rural population (165/1000) and unbooked cases (176 1000) as compared to urban population (92/ 1000) and booked cases (37/1000). The difference in either case was statistically significant (P <0.001).
The number of women who had one or more abortion was lower in the still-birth group (9. 6%) as compared to those, who gave birth to like children (13.7%).
Characteristics of still-births:
The characteristics of still-births have been shown in Table II.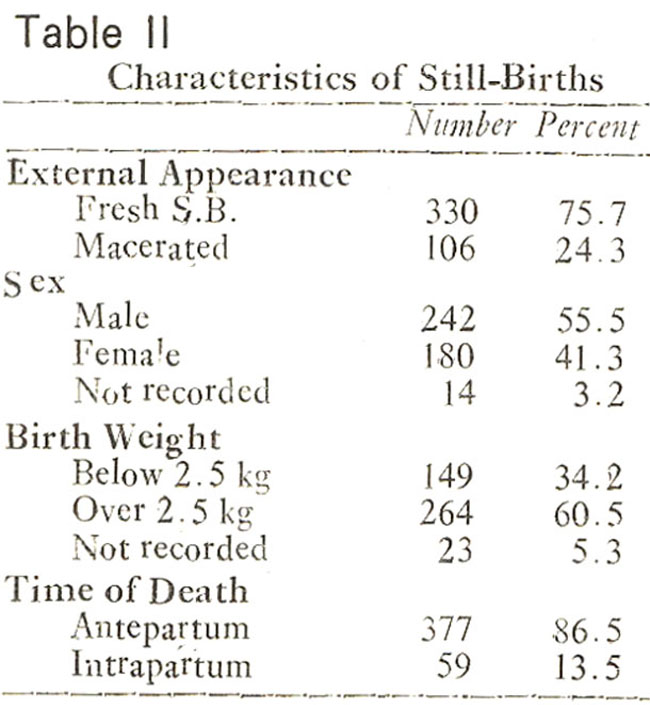
The majority of still-births (75.7%) were fresh and in 86.5% cases the fetus was dead at the time of admission. There was a preponderance of males (55.5%), the sex ratio being 1 .34. Only 34.2% of the still-births weighed 2.5 kg or The fetal heart sound was not heard at the time ofadmission in 86.5% cases, while in the rest death occurred during the process of labour.
The prevailing social norms of the society do not approve of post-mortum examinations and as such it is almost impossible to get parental consent for any such procedure. So one can only identify the factors associated with still-. However in 54 cases (12.2%) no definite factor could be identified. The possible factors have been summarised in Table III.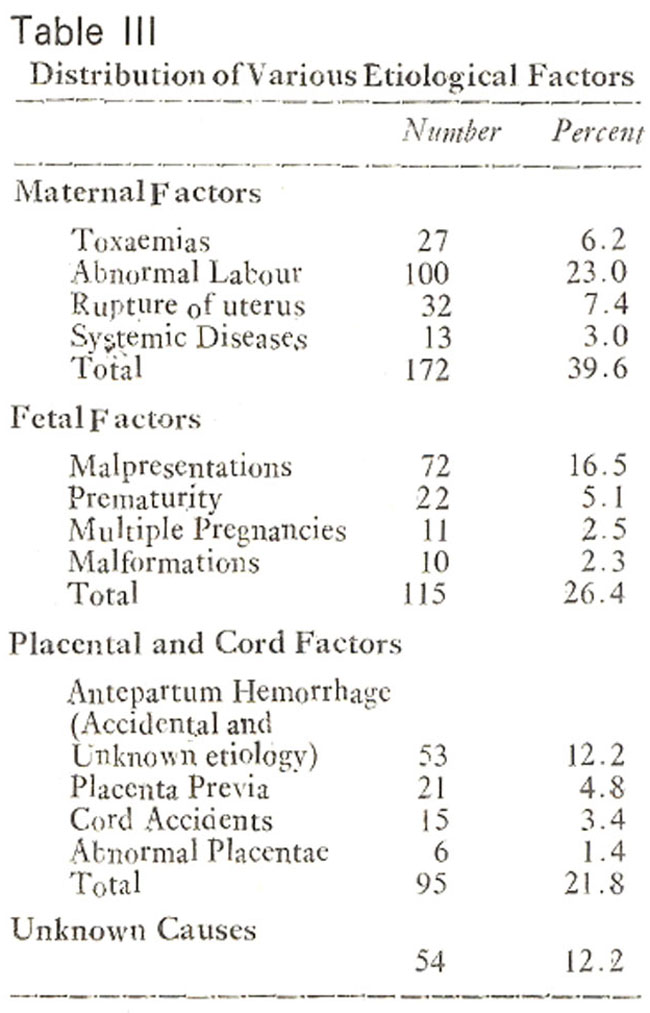
The most prominent were abnormal labour (23%), antepartum hemorrhage (17%) and malpresentations (16 5%). The term “antepartum hemorrhage” has been used to include placenta previa as well as accidental and unspecified antepartum hemrrhage.
Maternal factors:
There were 172 cases (39.6%) in which the cause of still-birth could be attributed to mother. Out of them 27 (6.2%) were due to toxaemias, 32(7.4%) due to the rupture of uterus, 13(3%) due to maternal diseases and 100 (23%) due to obstructed labours because of cephalo-pelvic dis-proportions (80.6%), contracted pelves (6.8%), shoulder dystocia (5. 1%), uterine inertia (3 .4%), complete vaginal septum (1 .7%), or other causes (2. 4%). The maternal diseases were one case of Hypertension (B.P. 180/120 mmHg), 3 cases of Hydramnios, 7 cases of Anaemia (Hb 5G/dl or below), one case of acute febrile illness and one case of afibirogenemia.
Fetal factors:
In the present series, 115 cases constituting 26.4% of the total still-births could be attributed to fetal factors. The maipresentatlons (16.5%) and prematurity (5.1%) were the most prominent factors. Out of the 72 cases of malpresentations, 52 were breech, 12 transverse lie, 6 compound presentation and 2 brow presentations. Twenty two children were premature i.e., horn before 37th week of gestation while 11 cases, 10 set of twins and 1 set of triplet, were the result of multiple pregnancies. Among 10 cases of congenital malformations, 4 were anencephalous, 1 hydrocephalous, 1 hydrocep- halous with spina bifida, 1 monster and 3 other minor malformations.
Placental and Cord factors:
Ninety five still-births (21 .7%) were due to placental or cord factors. Antepartum hemorrhage (A.P.H.) of accidental and unknown et iology (12 2) and placenta previa (4.8%) were the major causes. Among 15 (3.4%) cases of cord accidents, there was proplapse of cord in 4 cases, very short cord (8 cm and 11 cm) in 2 cases and in 9 cases the cord was tightly wrapped round the neck of the infant twice or thrice. The external appearance of all the abnormal placentae was that of a malarious placenta, though appropriate histological studies were not done. Out of six such cases 5 were found in primiparae.
Maternal MortaIity:
There were 21 maternal deaths in this series, giving a maternal mortality rate of 48/1000 deliveries. Six deaths were due to rupture uterus, 4 due to A.P.H, 3 due to eclampsia, 3 clue to maipresentation, and 5 due to obstructed labour.
Discussion
The stiIl-birth rate of 113/1000 birth is extremely high as compared to the developed countries. This may partly be due to the selectivity of hospital data. As pointed out in our previous paper (Rehan and Tafida, 1979), there is an inherent defect in relying on hospital data for biological standards of any community. However me studies of this nature will continue to be based on hospital data until compulsory and satisfactory vital statistical registration is introduced in developing countries. Unfortunately there are no studies from any part of Nigeria to compare with our data. Some authors (Harrison, 1978; Osuthor, 1976) have made occasional references to this problem. The former working in Zaria have stated a peri-ijatal death rate Of 88/1000 births while the interpolation of the data presented by the latter shows a still-birth rate of around 77/1000 singleton births. However the population studied by both these authors was a mixed population, comprising mainly of the non-Hausas and majority of the women were boolied cases. The other notable studies of still-births in African population are those of Ampofo from Ghana (1971) and Grech from Uganda (1967).
The findings of our study are in agreement with those of PMS as compared to any other study. In PMS when the effects of age and parity grouped together, the highest SBR was observed among women above 30 years or below 20 years, whereas in our series the highest rates were in women of 35 years and above or those of 16 years and below. The lowest SBR in PMS was among women of 25-29 years, while in our series the lowest rate was in 17-18 years age group. In either series the lowest SBR was among secundiparae and highest among those of parity 5 or above and the increasing birth order was related to higher still-birth rates. On the contrary the studies from Ghana and Uganda show that the highest SBR. was among the primiparac of 20-24 years and 19-23 years respectively. Apart from any other factors, which might be responsible for this difference, we have to first consider one statistical omission which both these authors have committed. In either of these studies, the age and parity-specific still. birth rates have been calculated as number of still-births in a particular age or parity group divided by the total number of still births. In strict epiderniological terms, this indicates the still-birth ratio and not the stillbirth rate, because to calculate any age or parity specific rate, if the numerator is confined to a certain age or parity, the denominator must also be similarly limited (McMahan and Pugh, 1970). Therefore we will restrict our comparison only to the etiological factors mentioned by them, but not to their age or parity specific still-birth rates.
The most prominent etiological factor in the present series was obstructed labour mostly due to cephalo pelvic disproportion particularly at the brim. Most of the women so effected, were younger than 20 years, and were admitted in the second stage of labour after many hours of trial at home. This view is also supported by the clinical studes of Libter (1960) from southern Nigeria who also found the cephalo-pelvic disproportion to be the most important cause of obstructed labour. Another factor associated with the obstruction of labour is shallowness of pelves in Nigerian women. The effective depth of true pelvis or the length of bony canal is a factor of importance in the mechanics of labour. However the pelvimetric studies carried out by Kolawale et al. (1978) have demonstrated that the pelves in Nigerian women are shallower than those of their caucasian counterparts as judged by significantly smaller straight sacral lengths and symphyseal measurements. The women studied by Kolawale et al. (1978), were all in third decade of life and thus their pelves were fully developed. I these fully developed pelves were smaller, then one can imagine the danger presented by a pelvis which is still growing as was the case in most of our subjects.
Malpresentations, though classified under fetal factors, also contribute to the causation of obstructed labour. Apart from prolonging the labour, particularly the second stage (Lister, 1960) malpresentations are known to be related to higher peri-na(al mortality b.y givig rise to intracranial damage and pulmonary complications (Fianu, 1976). The mean duration of labour in these cases was 26.4 ± 12 .0 hours whereas the mean duration of labour for normal delivery in local population is 19.5±9.8 hours. The difference was highly significant (P <0.001). The malpresentations were more common among women of parity 4 and above as compared to those of lower parities probably because of the lax multiparous uterus.
The rupture of the uterus, not a separate entity per se, is actually the sequelae of obstructed labour. The rupture may occur either from over-stretching of the lower segment or necroses from the pressure of presenting parts against the promontory of pelvis or a combination of both (Lister, 1960). Among this group only 2 cases (6.3%) were primiparae; all others were multipara; 14 (43.7%) being grand multipara, which confirms the common obstetrics belief that prolonged obstruction in primigravidae usually leads to secondary uterine inertia while in multiparae obsttüction is more likely to lead to uterine rupture.
The anterpartum hemorrhage accounted for about 17% of still-births. Since most of these cases are rushed to the hospital as emergencies, detailed investigations to arrive at a definite cause are not possible. Therefore we have preferred to include all such cases under one umbrella. The causal association of APH and 1)Iacenta previa with still-births is a well established fact (Clayton et al., 1972; Naeye, 1978; Knab, 1978). The over-all incidence of “Third Trimester Bleeding” in our series was lower than that reported by Ampofo (1971) from Ghana (20.5%) but higher than that quoted by Grech (1967) from Uganda (12.2%), though the incidence of placenta previa was almost identical in all three series. Fifty four percent of stillbirths associated with APH were among women of parity 5 and above, while only 17% cases were among primiparae and 6.2% in secondiparae. This is in comformity with the findings of Paintin (l962).
Toxaemias, both preieclamptic toxaemia and eclampsias, were associated with 27 cases of still-births, constituting 6.2% of the total still births. Toxaemias were common in women of younger age and lower parity, 75% cases being recorded among prirniparae of 18 years or below. The highest parity among toxaemia group was 4 in a woman aged 32 years. The incidence of toxaernia is lower than reported by Ampofo (1971) and Grech (1967).
The prolapse of the cord which occurred in4 cases was not associa,tecl with maipresentations. In all cases the length of the cord was normal, the presenting part was vertex, which was not engaged till the time of admission. The prolapse may be a sequelae of this late engagement of the head, which is very common in Nigerian women and has been attributed to the narrow sagital diameter and greater inclination of pelvic inlet (Kolawale et al., 1978). The prolapse of the cord has been found to be associated with stillbirths even in highly developed countries where immediate and adequate medical care is available (Migliorine and Pepperell, 1977). The short cord can cause fetal death by delaying the descent of head, thus making the delivery difficult (Bailey, 1972) or by exerting traction. The association of a malarious placenta and stillbirth has been well established by Lawson and S;ewart (1976). Although the exact mechanism involved is not clear, yet the anemia resulting from repeated attacks of malaria and the placental insufficiency due to placental parasitization have been stated as causative factors. It would appear that the parasitized cells tend to sludge in the eddies of the slow moving placental stream and most probably favour fibrin deposition on the villi, thus hastening the degenerative processes, interfering with nutrition of the fetus and causing stillbirths or premature labout(Edington and Gilles, 1976).
Apart from these clinical observations, we are tempted to think that some sociological factors may also be contributing to this extremely high SBR. One social factor, which has been proved to be of etiological importance for fetal wastage is the age difference between the spouses.
The studies by Awan and Mobashar (1975) and Selvin and Garfinkel (1976) have clearly demonstrated that the fetal wastage increases proportional to the age difference between the spouses. Because of the practice of polygamy among the local population, there is usually a big difference between the age of husband and that of his subsequent wives.
A recent survey carried out among the urban and rural populations of this area shows that the latest wives are usually 13.49+-4 58 years younger than the husband (Unpublished data). In some cases the difference was as high as 40 years.
Another factor of social importance is the role of traditional medicine. In the present series 17 women (3 9%) gave a history of taking traditional medicine. Though the phar-macological analysis of these drugs was not carried out, yet these are believed to have oxytocic effect (Lawson and Stewart, 1976). Similar findings have been reported from Uganda by Grech (1967) who states that patients taking these drugs believed that these will shorten the duration of labour and according to him the analsis of these drugs at pharmacology depaftment of his hospital has proved that some of these herbs have a definite oxytocic action.
Due to the lack of data regarding the height of the population studied, the effects of this paraneter on still-birth rates could not be evaluated. The number of those women, who smoke was too small to merit any valid analysis.
Acknowledgements
We are grateful to Dr. K. Balasingharn, Senior Consultant Gynaecologist, Maternity Hospital Katsina, for permitting an access to the records. Special thanks are due to Miss Priscilla Nwoke for secretarial help and to Mrs. Rehan for her encouragement and helpful review of the manuscript.
References
1. Adamu, M. The Hausa factor in West African History. Zaria, Ahmadu Bello University Press, 1978, pp. 1-4.
2. Ampofo, D.A. (1971) Stillbirth and its prevention in Ghana. Ghana Med. J., 10:123.
3. Awan, A.K. and Mobashar, M. (1975) Age differential between spouses and pregnancy wastage. JPMA., 25:46.
4. Bailey, R.E. Maye’s midwifery; a textbook for midwives. 8th ed. London, Bailliere, 1972.
5. Butler, N.R. and Atberman, E.D. Perinatal problems. London, Wilicams and Wilkins, 1969.
6. Clayton, S., Fraser, D. and Lewis, T. Obstetrics. 12th ed. London, Arnold, 1972.
7. Fianu, S. (1976) Fetal mortality and morbidity following breech delivery. Acta Obstet. Gynecol. Scand., 56 (Supp) 7.
8. Grech, E.S. (1967) Stillbirths in Uganda. Obstet. Gynaecol, 29:764.
9. Greenhill, J.P. Biological principles and modern practice of Obstetrics. Philadelphia, Saunders, 1974, P. 457.
10. Harrison, K. (1978) Child bearing in Zaria. New Nigerian, 3870:28.
11. Hill, P. Rural Flausa; village and a setting, Cambridge, University Press, 1977.
12. Hughes, E. Obstetric gynaccologic terminology. Philadelphia, Davis, 1972.
13. Knab, D.R. (1978) Abruptio placental; as assessment of the time and method of delivery. Obstet. Gynecol., 52 :625.
14. Kolawale, T.M., Adamu, S.P. and Evans, K.T. (1978) Comparative pelvimetric measurements in Nigerian and Welsh Women. Clin. Radiol., 29:85.
15. Lawson, J.R., Stewart, D.B. Obstetrics and gynaecology in the tropics and developing countries. 2nd ed. London, Arnold, 1976.
16. Lister, U.G. (1960) Obstructed labour; a series of 320 cases occuring in 4 years in a hospital in Southern Nigeria. J. Obstet. Gynaec. Brit. Emp., 67:188.
17. Madauci, I., Isa, Y. and Daura, B. Hausa Customs. Zaria, Northern Nigerian Publication Company, 1968, pp. 18-20.
18. McMahan, B. and Pugh, T. Epidemiology, principles and methods. Boston, Little Brown and Company, 1970.
19. Migliorine, G.D. and Pepperell, R.J. (1977) Prolapse of the umblical cord; a study of 69 cases. Mea. J. Aust., 2:522.
20. Naeye, R.L. (1978) Placenta previa; predisposing factors and effects on the fetus and surviving infants. Obstet. Gynecol. 52:521.
21. Osuthor, D. (1976) Birthweights in Malumfashi, North Central State of Nigeria. Niger Med. J., 6:327.
22. Paintin, D.B. (1962) The epidemiology of ante-partum hemorrhage; a study of all births in a community. J. Obstet. Gynaecol. Brit. Common., 69:614.
23. Rehan, N. and Tafida, DS. (1979) Birthweight of Hausa infants in northern Nigeria. Br. J. Obstet. Gynaecol., 86 :443.
24. Rehan, N. and Tafida, D.S, (1980) Multiple births in Hausa women. Br. J. Obstet. Gynaecol., 87:997.
25. Rehan, N. and Tafida, D.S. (1981) Low birthweight in Hausa infants. NIg. J. Paediatr., 8:35.
26. Rehan, N. and Abashiya, ASK. (1981) Breast-feeding and abstinence among Hausa women. Stud. Fam. Plann., 12:233.
27. Selvin, S. and Garfinkel, J. (1976) Paternal age, maternal age and birth order and risk of a fetal loss. Hum. Biol., 48:223.
28. Smith, A. The early states of the Central Sudan, in history of West Africa, Edited by J.F.A. Ajayi and Mcrowder. London, Longman, 1976, pp. 177-198.
29. World Health Organisation (1950) Expert committee on health statistics; reportion the second session, Geneva, 18-21 April, 1950. WHO. Tech. Rep. Ser., 25:1.
30. World Health Organisation (1961) Public health aspects of low birth weight; third report of the expert committee on maternal and child health. WHO. Techn. Rep. Ser., 217:3.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: