
Saleha Anwar ( Department of Radiology, Liaquat National Hospital and Medical College, Karachi. )
Bushra Rehan ( Department of Radiology, Liaquat National Hospital and Medical College, Karachi. )
Gulzar Hameed ( Department of Radiology, Liaquat National Hospital and Medical College, Karachi. )
February 2014, Volume 64, Issue 2
Original Article
Abstract
Objective: To determine the diagnostic accuracy of magnetic resonance imaging in ultrasonographically indeterminate masses of female pelvis against histopathological findings.
Methods: The comparative cross sectional, analytical study was conducted at Liaquat National Medical College and Hospital, Karachi, from January to December 2006. Female patients with pelvic masses in whom the definite diagnosis of the mass could not be determined by ultrasonogaraphy were further evaluated with magnetic resonance imaging of the pelvis. All patients subsequently underwent a surgical procedure for a definite histopathological diagnosis. The imaging results were then compared with the pathological results to determine the sensitivity and specificity of magnetic resonance imaging for the determination of the nature of mass and anatomical site of the origin of mass.
Results: The age of the 63 patients in the study ranged between 14 and 84 years. The sensitivity and specificity of the imaging procedure for the assessment of benign lesion was 95.8% and 93.3% respectively, and for malignant lesion, 93.3% and 95.8% respectively. In diagnosing uterine mass, the values were 100% and 97.5% respectively, for ovarian mass, 97.3% and 96% respectively, and extra uterine/extra ovarian mass, 66.6% and 100% respectively.
Conclusion: Magnetic resonance imaging was highly accurate in characterising the pelvic masses as benign and malignant and in determining their site of origin.
Keywords: Magnetic Resonance Imaging, Female pelvis, Indeterminate masses. (JPMA 64: 171; 2014)
Introduction
The main goal of imaging in the evaluation of an adnexal mass is the detection of malignancy.1 Magnetic resonance imaging (MRI) is an accepted imaging method for diagnosing diseases of the female pelvis.2-4 It has been shown to have potential in the characterisation of adnexal masses and has emerged as a cost-effective technique for the evaluation of a variety of disorders of the female pelvis, including endometriosis and cervical cancer.5-7 MRI of the pelvis in some clinical situations can obviate surgery, change a planned surgical procedure, alter medical treatment, and decrease healthcare costs, particularly after an inconclusive sonogram of the adnexa has been obtained.8-10 The objective of the current study was to evaluate the role of MRI in the characterisation of female pelvic masses. Although similar studies have been conducted by other researchers, but we believed it was important to conduct it again for two reasons. Firstly, the cumulative numbers of other such studies are small which makes every new paper a useful addition to the literature. Secondly, to the best of our knowledge, none of the studies have been reported from our region, which makes it not only the first regional report of its kind, but might also add a fresh perspective to the existing literature.
Patients and Methods
The comparative, cross-sectional study was conduted at Liaquat National Medical College and Hospital, Karachi, from January to December 2006. All female patients presenting with previously performed ultrasound showing indeterminate pelvic mass where a definite diagnosis of the mass could not be determined by ultrasonogaraphy, and without a histopathological diagnosis were included in the study. For patients under the age of 18, consent was acquired from their legal guardians, and for those above the age of 60, if they were in a mental state in which they could make their own decisions, they gave consent themselves. Otherwise, the legal guardians gave consent on their behalf.
Patients who were not a candidate for surgery for histopathological confirmation of their pelvic mass were excluded. All patients underwent an MRI evaluation of their pelvis, which was compared with subsequent histopathological diagnosis.
MRI were obtained with standard protocol requiring 6 hours fasting, empty bowels and full bladder. 1.5-T MRI with a flexed body array in supine position was used. Immediately before MRI, all patients were given 1mg of intramuscular glucagon. None of the patients had contraindications to the administration of glucagon. Total imaging time was 25 minutes and images obtained were: Sagittal and Axial T2-weighted fast spin-echo images; Axial T1-weighted spin-echo images; Axial T2-weighted spin-echo images through any lesion images with the addition of frequency-selective fat suppression; and Coronal T2-weighted fast spin-echo images.
Contrast enhanced images were immediately obtained after injecting intravenous (IV) gadolinium at a dose of 0.1mmol/kg of body weight (maximum 20ml). MRI reporting was done by two independent qualified radiologists, blinded to each others\' findings. Masses were characterised based on various factors such as thickness and enhancement of walls, internal enhancement, thickness of septae more than 3mm, presence of mural nodule and papillary projections, as well as on signal characteristics. Data was initially collected on standardised pre-tested proformas, and later shifted to SPSS version 10. Data was utilised to calculate sensitivity, specificity, positive and negative predictive values (PPV and NPV) for both benign and malignant masses and also for specific anatomical site of the origin of mass. The gold standard was histopathology.
Results
Initially 71 patients had be enrolled, but 4 (5.63%) were excluded as there was no mass found on MRI examination, and 4 (5.63%) were lost to follow-up. The final number of patients comprising the study group was 63 (88.73%). The ages ranged from 14 to 84 years with a mean age of 40±13.69 years. Correct assessment of benign and malignant masses was made in 60 (95.23%) patients. Out of the remaining 3 (4.77%) patients, 2 (3.27%) were reported to be malignant on MRI, but turned out to be benign on histopathology, and 1 (1.58%) was reported to be benign and turned out to be malignant. On final histopathological analysis, 48 (76.19%) cases were proven to be benign, out of which 46 (73%) were correctly diagnosed on MRI, while 15 (23.8%) cases were proven to be malignant, out of which 14 (22.2%) were correctly diagnosed on MRI. Out of 14 malignant masses, there were 5 (35.7%) solid malignant ovarian tumours, 8 (57.14%) were solid-cum-cystic masses, out of which 4 (50%) showed papillary projections. Enhancing thick septae were present in 6 (75%) cases. Two (3.27%) cases, which were reported as malignant masses, turned out to be complicated haemorrhagic ovarian cyst and broad ligament fibroid (Table-1).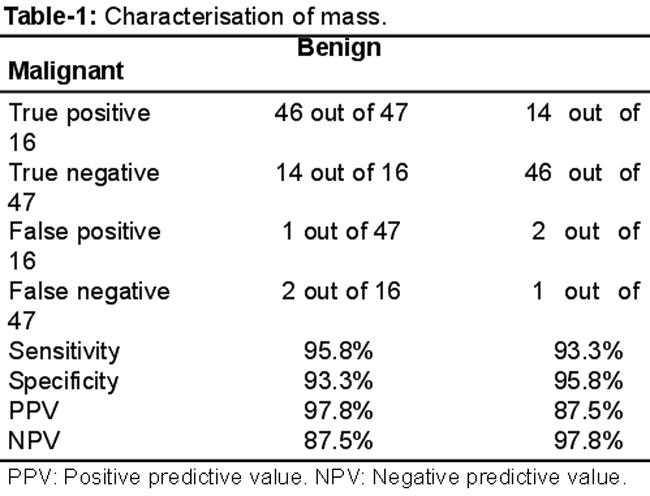
Correct assessment of the site of origin of mass was made in 61 (96.82%) patients. Out of 63 total cases, 23 (36.5%) masses were reported to be uterine in origin on MRI. Of these, 22 (95.65%) were confirmed on histopathology, while 1 (4.35%) was incorrectly characterised. Out of 41 extra-uterine masses, 38 (92.68%) were reported as ovarian in origin; 37 (97.36%) of these turned out to be ovarian on histopathology, while 1 (2.63%) was incorrectly characterised. Out of 3 extra-uterine and extra-ovarian masses, 2 (66.6%) were correctly diagnosed on MRI, while the remaining 1 (33.3%) was incorrectly reported as an ovarian mass (Table-2).
Discussion
In the initial evaluation of pelvic masses, ultrasound has become the imaging modality of choice because of a number of reasons. First, it is easily available. Secondly, it is inexpensive. Moreover, it is a safe and quick method for the assessment of female pelvic masses. Despite its popularity and widespread acceptance as first-line imaging modality, there are times when ultrasound fails to determine the origin, extension and characteristics of female pelvis masses i.e. benign or malignant. Such female pelvic masses which are difficult to characterise on the basis of ultrasound alone have been termed "indeterminate pelvic masses".1 It is in such situations that MRI is fast growing as the imaging modality of choice following ultrasound.11
Our study focused on the viscera of origin and lesion characterization (benign vs. malignant). We used the imaging technique described in literature using coronal T2-weighted fast spin echo, axial T1-weighted spin echo, sagittal T2-weighted fast spin echo images and pre and post contrast T1-weighted fat suppressed images.1 Previously, Mitchell et al found that the coronal plane is most useful because it depicts the anteverted uterus in cross-sections.12 Dooms et al on the other hand suggested that the combination of coronal and axial planes is most useful in determining the site of origin of the pelvic mass.13 Other investigators have also used only sagittal and axial planes for imaging, without coronal sections, which were once rarely used.14,15 We decided to use all three imaging sequences as well as contrast parametres that were used and advocated by Adusumilli et al.1
Our study featured 15 histopathologically proven malignant masses out of which MRI accurately picked up 14, giving a sensitivity of 93.3%. The only false negative was the ovarian carcinoma of a middle-aged female incorrectly categorised as a pedunculated fibroid with areas of cystic degeneration.16 The mass was in close proximity with the uterus and showed diffuse high signals on T1-weighted images and variable signals on T2-weighted images. There was no supportive evidence of enlarged nodes or presence of ascites to label this case as malignant. Considering the age of the patient and signal intensities demonstrated on T1 and T2-weighted images, this particular case was reported as pedunculated fibroid with degeneration. Chang et al in their study reported nine leiomyomas with degeneration (9/52) which on T1-weighted images were heterogeneous and showed areas that were high on T1 and T2-weighted sequences.17 We based our diagnosis in this particular case on Chang et al\'s observations. For the diagnosis of malignant lesions, when we compare our overall result of 93.3% sensitivity with other similar studies, Adusumilli et al have shown 100% sensitivity in diagnosing malignant lesions, but their sample size only comprised five malignant cases compared to our 15. Our results, however, are comparable to the results obtained by Hricak et al who showed sensitivity of 95% in depicting malignancy in such cases.1,11
Our study also featured 48 histopathologically proven benign masses out of which MRI accurately picked up 46, giving a sensitivity of 95.8% and specificity of 93.3%. Of the other two masses, one was a complicated adnexal mass in a young woman demonstrating thick septas, thick enhancing walls and mixed signal intensities on T1 and T2-weighted images. As both ovaries were not visualized, this case was reported as an ovarian carcinoma, but it turned out to be a complicated haemorrhagic and infected ovarian cyst on histopathology. Another was a solid adnexal mass in a post-menopausal woman showing intermediate signal intensities and intense enhancement after post-contrast study; two features suggestive of malignancy.1 It was a broad ligament fibroid on histopathology. For the diagnosis of benign lesions, Scoutt et al showed a specificity of 94% that is similar to our own results.18
While determining the site of origin, we studied different viscera separately and compared our results with other investigators. In case of detection of uterine origin of masses, our study showed sensitivity of 100% in 22 patients, and in this regard our results are comparable with the works of Scoutt et al and Adusumilliet al.1,18 Similarly, in case of detection of ovarian origin of masses, we found the sensitivity of MRI to be 97.3% in 38 patients. Adusumilli et al in their study obtained a sensitivity of 98%, and our results were thus in accordance with their work.1 A solid mass adjacent to the uterus can be a pedunculated fibroid or an adnexal mass. Usually their differentiation is straightforward, but the appearance of a pedunculated fibroid may simulate that of a solid adnexal mass.19 In our study there were 19 numbers of such cases out of which 14 (73.6%) turned out to be pedunculated fibroids, while the rest were histopathologically proven ovarian masses (26.3%).
Our findings that MRI is helpful in determining the site of origin of these masses and characterisation as benign or malignant are also similar to the results of Weinreb et al.14 However, they used a smaller sample size and focussed only on patients with solid pelvic masses, while our study had a larger sample size and consisted of all types of pelvic masses of indeterminate origin, both solid and cystic. We also had three histologically proven extra-uterine and extra-ovarian masses out of which two were correctly diagnosed on MRI as paratubal cysts, while one fibroid of broad ligament was incorrectly categorised as solid ovarian mass.1
Conclusion
MRI is highly accurate in characterising pelvic masses as benign or malignant, and in determining their site of origin. No inter-observer variability between the two radiologists was noted. MRI might not offer any additional information in characterising unilocular cystic ovarian lesion, but for large solid or cystic pelvic masses, complex adnexal masses, or a questionable large pedunculated fibroid versus ovarian malignancy, MRI is extremely helpful.
References
1. Adusumilli S, HussainHK, Caoili EM. MRI of Sonographically Indeterminate Adnexal Masses. Am J Roentgenol 2006; 187: 732-40.
2. Hricak H. Current trends in MR imaging of the female pelvis. Radiographics 1993; 13: 913-9.
3. Chang YC, Hricak H. Current status of MR imaging of the female pelvis. Crit Rev Diagn Imaging 1989; 29: 337-56.
4. Hricak H. MRI of the female pelvis: a review. Am J Roentgenol 1986; 146: 1115-22.
5. Yu KK, Hricak H. Can MRI of the pelvis be cost effective? AbdomImag 1997; 22: 597-601.
6. Sugimura K, Imaoka I, Okizuka H. Pelvic endometriosis: impact of magnetic resonance imaging on treatment decisions and costs. Acta Radiol 1996; 3: 66-8.
7. Hricak H, Powell CB, Yu KK. Invasive cervical carcinoma: role of MR imaging in pretreatment work-up-cost minimization and diagnostic efficacy analysis. Radiology 1996; 198: 403-9.
8. Schwartz LB, Panageas E, Lange R, Rizzo J, Comite F, McCarthy S. Female pelvis: impact of MR imaging on treatment decisions and net cost analysis. Radiology 1994; 192: 55-60.
9. Yamashita Y, Hatanaka Y, Torashima M, Takahashi M, Miyazaki K, Okamura H. Characterization of sonographically indeterminate ovarian tumors with MR imaging: a logistic regression analysis. ActaRadiol 1997; 38: 572-7.
10. Medl M, Kulenkampff KJ, Stiskal M, Peters-Engl C, Leodolter S, Czembirek H. Magnetic resonance imaging in the preoperative evaluation of suspected ovarian masses. Anticancer Res 1995; 15: 1123-5.
11. Hricak H, Chen M, Coakley FV. Complex adnexal masses: detection and characterization with MR imaging-multivariate analysis. Radiology 2000; 214: 39-46.
12. Mitchell DG. Chemical shift magnetic resonance imaging: applications in the abdomen and pelvis. Top Magn Reson Imag 1992; 4: 46-63.
13. Dooms GC, Hricak H, Tscholakoff D. Adenexal structures: MRI. Radiology 1986; 158: 639-42.
14. Weinreb JC, Barkoff ND, Megibow A, Demopoulos R. The value of MR imaging in distinguishing leiomyomas from other solid pelvic masses when sonography is indeterminate. Am J Roentgenol 1990; 154: 295-9.
15. Kim JC, Kim SS, Park JY. "Bridging vascular sign" in the MR diagnosis of exophytic uterine leiomyoma. J Comput Assist Tomogr 2000; 24: 57-60.
16. Hricak H, Tscholakoff D, Heinrichs L, Fisher MR, Dooms GC, Reinhold C. Uterine leiomyomas: correlation of MR, histopathologic findings and symptoms. Radiology 1986; 158: 385-91.
17. Chang, Cooperberg PL, Wong AD, Llewellyn PA, Bilbey JH. Limited-sequence magnetic resonance imaging in the evaluation of the ultrasonographically indeterminate pelvic mass. Can Assoc Radiol J 2004; 55: 87-95.
18. Scoutt LM, McCarthy SM, Lange R, Bourque A, Schwartz PE. MR evaluation of clinically suspected adnexal masses. J Comput Assist Tomogr 1994; 18: 609-18.
19. Shoaib SA, Sahdev A, Van Trappen, Jacobs IJ, Rezenk RH. Characterization of adnexal mass lesion on MR imaging: a logistic regression analysis. Acta Radiol 1997; 38: 572-7.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: