
Kulsoom Farhat ( Department of Pharmacology and Therapeutics, Army Medical College, National University of Sciences and Technology, Rawalpindi, Pakistan. )
Anwar Kamal Pasha ( Department of Anaesthesiology, Combined Military Hospital, Rawalpindi, Pakistan. )
Nusrat Jaffery ( Department of Pharmacology and Therapeutics, Army Medical College, National University of Sciences and Technology, Rawalpindi, Pakistan. )
February 2014, Volume 64, Issue 2
Original Article
Abstract
Objective: To evaluate the biochemical changes associated with succinylcholine administration after pretreatment with rocuronium at different time intervals.
Method: The prospective, randomised, single-blinded study was conducted at the Combined Military Hospital, Rawalpindi, from January to May 2010. Ninety male, aged 18-60 years, American Society of Anaesthesiology I or II patients undergoing elective inguinal herniotomy or external haemorrhoidectomy were included. The patients were randomly divided into three equal groups. Group A received a normal saline 5ml as placebo 1 minute before succinylcholine; Group B received rocuronium 0.06 mg/kg 1 intravenously minute before succinylcholine, while Group C received intravenous injection of rocuronium 0.06 mg/kg 5 minute before succinylcholine. Venous blood samples for creatinine phosphokinase, lactate dehydrogenase and myoglobin plasma concentrations were obtained at 0, 30 minutes, 6 hours and 24 hours after succinylcholine administration.
Results: Mean serum creatinine phosphokinase and myoglobin concentrations were significantly decreased in Groups B and C compared to Group A at 30 minutes and 24 hours (p<0.05). However, no significant difference in the enzyme levels at any time interval was observed among the rocuronium groups. There was a significant rise in lactate dehydrogenase concentrations at 6 hours and 24 hours in Group A compared to Groups B and C (p<0.05).
Conclusion: Pretreatment with rocuronium effectively reduces the biochemical changes associated with succinylcholine-induced muscle fasciculations. However, whether it is given 1 minute or 5 minutes before succinylcholine does not make much difference.
Keywords: Succinylcholine, Rocuronium, Creatinine phosphokinase, Lactate dehydrogenase, Myoglobin. (JPMA 64: 146; 2014)
Introduction
Patients undergoing surgical procedures under general anaesthesia usually need endotracheal intubation. While various neuromuscular blocking agents (NMBA) can be used for this purpose,1 succinylcholine is still one of the most widely used drugs in our setup due to its rapid onset of action, short duration of action and especially its lower cost.2 However, it produces some undesirable side effects such as muscle fasciculations, post-operative myalgias, increased serum levels of creatinine phosphokinase (CK), lactate dehydrogenase (LDH), myoglobin and potassium.3
Succinylcholine-induced fasciculation are the involuntary skeletal muscle contractions caused by transitory stimulation of some muscle fibres that occur few seconds after the administration of the drug.3 Commencing with the contractions of the muscles of eyelids, they quickly spread over the face and neck to the trunk. It is suggested that these fasiculations result in the postoperative myalgias and release of CK from muscle fibres resulting in a rise of the blood CK levels.4 A marked rise in the level of serum CK is associated with tissue trauma during surgery that occurs postoperatively with maximal level recorded at 24 hours after operation, followed by a decrease towards the normal level within five days.5 Likewise, there is enough evidence that myoglobin levels also increase after the administration of succinylcholine.6 Such muscular untoward effects in the form of fasciculations, myalgias and biochemical changes limit the usefulness of succinylcholine.7 Nevertheless, despite all these adverse effects succinylcholine still remains one of the most widely used drugs in the developing countries, such as Pakistan, mainly due to its lower cost, the most rapid onset of action, shortest duration of action and the most reliable and intense skeletal muscle paralysis compared to the other neuromuscular blockers.2,8 It is a drug of choice in Rapid Sequence Intubation in ICU during medical and surgical emergencies and trauma surgery.
Even though a large numberof NMBAs have been used in recent times, so far these drugs could not challenge the relentless persistence of succinylcholine in our anaesthetic practice.
Rocuronium is a non-depolarizing NMBA. It is used in modern anaesthesia to facilitate endotracheal intubation.8,9 A more rapid onset of action compared to other non-depolarising agents delivers good intubating conditions within 60-90 seconds2,3 of its administration. In certain recent studies, the effectiveness of pretreatment with rocuronium in reducing the muscular adverse effects of succinylcholine2,8,10 has been statistically proven.
There has been a great deal of argument among the researchers about the interval between the non-depolarising muscle relaxant (NDMR) pretreatment and the administration of succinylcholine for endotracheal intubation since this interval may affect the efficacy of pretreatment.2,11 Although intervals of 2, 3, 4 min or even greater have been suggested,12 but researchers recommend 30 seconds, 1 min and 4 min time interval which can be safely applied for pretreatment with NDMR to prevent succinylcholine-induced muscular effects.2,8,9,12,13 These intervals are recommended keeping in view the fact that shorter intervals do not inhibit fasiculations while longer intervals offer no additional advantage.8,12
The aim of the present study was to assess the effectiveness of rocuronium pre-treatment 1 min and 4 min before the administration of succinylcholine and measuring succinylcholine-induced enzyme elevations, during thiopental-sevoflurane anaesthesia. Since Pakistan, like other developing states, is a poor country, an effort was needed to curtail the ever increasing expenses in providing healthcare facilities to the poor. Therefore, the current study was conducted with the aim of establishing that if the adverse effects of succinylcholine could be controlled with the technique of precurarisation with rocuronium, succinylcholine can still be used due to its various advantages.
Patients and Methods
The prospective, randomised, single-blinded study was conducted at the Combined Military Hospital, Rawalpindi from January to May 2010, after approval of the study project by the Ethical Committee of Centre for Research in Experimental and Applied Medicine (CREAM), Army Medical College, Rawalpindi. A total of 90 adult American Society of Anaesthesiology (ASA) I or II, Mallampati I patients undergoing inguinal hernioplasty or external haemorrhoidectomy were included in the study. Keeping in view the potential adverse effects of the drug, only patients who were relatively healthy and therefore less at risk were incuded drug under study. Moreover, short-duration surgical procedures were opted for. Written informed consent was taken. The patients were randomly divided into three equal groups according to a pretreatment plan.2 Group A received 0.9% saline 5ml intervenous (IV)1 min before succinylcholine; Group B received inj rocuronium 0.06mg/kg IV 1 min before succinylcholine, while Group C received inj rocuronium 0.06mg/kg IV 5 min before succinylcholine administration. Before that, all the patients were premedicated with inj pethidine 1 mg/kg IV just prior to surgery and pre-oxygenated with 100% oxygen for 3-5 minutes with a standard anaesthesia face mask. Anaesthesia was induced with inj thiopentone sodium 5mg/kg IV. Inj succinylcholine 1.5 mg/kg IV was given for endotracheal intubation. Anaesthesia was maintained with volatile anaesthetic agent sevoflurane and 60% nitrous oxide in oxygen. Monitoring of non-invasive blood pressure at 3min intervals, continuous pulse-oximetry, electrocardiography (ECG), capnography, temperature monitoring were carried out during the perioperative period. At the end of the procedure, sevoflurane was discontinued, NMBAs were pharmacologically reversed with inj neostigmine bromide 0.05mg/kg IV in atropine sulphate 0.02mg/kg. The patients were ventilated with 100% oxygen till consciousness was regained and the patients started following verbal commands. Endotracheal tube was removed after gentle suction of secretions. All the patients remained haemodynamically stable during anaesthesia while recovery from anaesthesia was smooth and uneventful. After ensuring full consciousness in the recovery room, the patients were shifted to the ward.
A total of four venous blood samples were taken for the measurement of serum CK, LDH and myoglobin concentration at 0 hours (at the time of administration of succinylcholine), 30 minutes, 6 hours and 24 hours after the administration of inj succinylcholine. Serum CK was measured by UV-Kinetic method at the Armed Forces Institute of Pathology (AFIP). LDH was measured using an ultraviolet (UV) — Kinetic method at AFIP. Myoglobin was measured using a two-site chemiluminescent enzyme immunometric assay method with an immulitemyoglobin kit.
The data was analysed using SPSS-13. Descriptive statistics were used to describe the data. Mean and standard deviations were used to describe quantitative variables like age, weight, duration of anaesthesia, duration of surgery, CK, LDH and myoglobin. Frequency along with percentage was used to describe qualitative variables like gender. Quantitative variables were compared through analysis of variance (ANOVA) between the groups. Paired sample t-test was used to compare values of CK, LDH and myoglobin within the groups. Chi-square test was used to compare qualitative variables between the groups. P<0.05 was taken as statistically significant.
Results
All the three groups were comparable with respect to age, weight and durations of anaesthesia and surgery (p<0.05) (Table).
The highest levels of myoglobin venous blood concentration were observed at 30 min after succinylcholine administration (p<0.01) (Figure-1).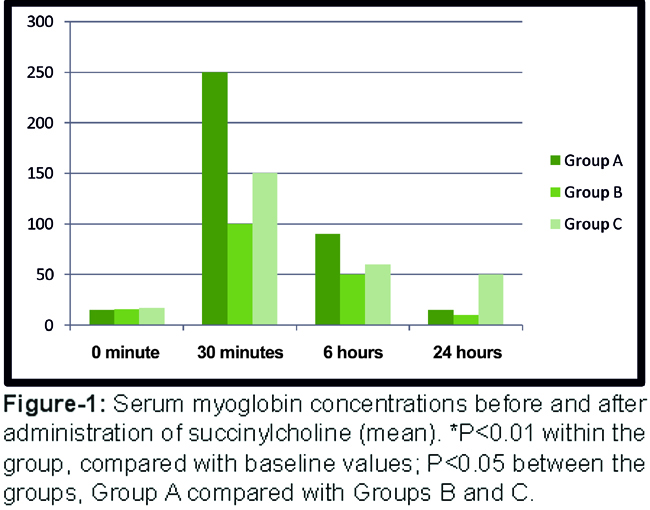
It was also observed that the patients in Group A showed a significantly higher rise in myoglobin concentration as compared to the other groups at this time (p<0.05). However, the difference between Group B and Group C at 30 minutes interval was statistically insignificant (p>0.05).
The highest levels of CK venous blood concentration were observed at 6 hours in all the three groups (p<0.05) (Figure-2).
However, Group A showed a significantly higher rise in CK than the others at 6 hours and 24 hours (p<0.05). Mean CK venous blood concentrations were also higher in Group A compared to Group B (p<0.05). There was a significant difference between Groups A and B, as well as between A and C at 6 hours and 24 hours, but there were no statistically significant differences between Groups B and C.
No statistically significant difference in LDH venous blood concentration between Group B and C was observed at 0 minute, 30 minutes, 6 hours and 24 hours (p>0.05) (Figure-3).
However, there was a significant increase in the mean LDH concentration in Group A at 6 hour and 24 hours compared to the other groups (p<0.05).
Discussion
Succinylcholine, the only depolarizing muscle relaxing agent in clinical use, is well-known for its most rapid onset of action and short duration of action2,8,9 compared to the NDMR dugs.14 It has been the most commonly used drug for the endotracheal intubation in the past. However, its popularity has reduced in recent modern anaesthesia practice, especially in the developed countries, due to the muscular adverse effects related to the drug.6,9 Nonetheless, the drug is still extremely useful in saving precious lives during various emergency clinical situations when a rapid endotracheal intubation is required. It is also a very useful drug in the Rapid Sequence Induction technique, especially when a difficult airway is also anticipated due to its quick onset and short duration of action. Furthermore, due to the low cost, it is still a very useful drug in developing countries such as Pakistan.1,2,5,8
It has been observed that succinylcholine increases the biochemical markers of muscle damage when administered during halothane or enflurane anaesthesia.5,8,12 However, the effect is less frequent during sevoflurane anaesthesia.15 Therefore, we used sevoflurane for the maintenance of anaesthesia in our study. The skeletal muscle injury is the main cause of the rise in myoglobin, CK, LDH during surgery. Since the muscle damage during various surgeries also results in a rise of these biochemical markers, patients undergoing inguinal herniotomy or hemorrhoidectomy procedures with minimal muscle damage16 were included in our study, so that our results are least affected. Similarly, intramuscular injections were intentionally avoided pre-operatively, and post-operative analgesia was given by the IV route. Therefore, the rise in enzymes levels in our study most likely reflected the effects of the NMBAs. We believed that if the untoward muscular side-effects of the drugs could be prevented, succinylcholine could still be used successfully since it is the least expensive NMBA. Furthermore the unmatched properties of quickest onset, shortest duration of action, most reliable and profound muscle relaxation, and not requiring reversal agent attributed to succinylcholine is unmatched with any other muscle relaxant in clinical use.
Pretreatment with a small dose of NDMR is considered to be almost the gold standard in the prevention of succinylcholine-induced muscular adverse effects. However, since pretreatment reduces the efficacy of succinylcholine, a higher dose is subsequently recommended.10,11,13 Therefore, we used the upper safe limit of the recommended dose of 1.5mg/kg in our study in order to achieve the ideal intubation conditions.
Much argument has been carried out among the researchers about the interval between administration of the NDMR drug for pretreatment and succinylcholine.2,11 Intervals of 2, 3, and 4 minutes or even larger have been recommended12. Such long intervals are recommended due to the shorter onset of NDMRs.
Rocuronium is an intermediate duration non-depolarising NMBA that has a more rapid onset of action than the other agents.6 Successful intubation can be achieved within 60 sec of its administration. It is the most commonly used drug for pretreatment since it reduces the incidence of succinylcholine-induced muscular effects much effectively than the other non-depolarizing agents.12,14 We used the recommended dose of 0.06mg/kg of rocuronium for pretreatment,12 1 minute and 4 minutes before the administration of succinylcholine. We observed that rocuronium pretreatment rapidly prevents succinylcholine-induced fasiculations within short interval because of rapid onset of action, and concluded that this time interval should be as short as possible to allow a busy operating list to proceed smoothly and should be long enough to allow sufficient effect.
It has been established that pretreatment with rocuronium is also effective in reducing the rise in serum myoglobin and CK concentrations compared with patients pre-treated with other drugs such as vecuronium, mivacurium, atracurium, midazolam, or patients who received succinylcholine alone.15-17 In the present study, we also observed that pretreatment with rocuronium effectively reduced the succinylcholine-induced myoglobin and CK elevations. Similar results were also observed by some other investigators.8,10,12
It was also noted that the levels of LDH were raised at the different intervals of sampling in our study with succinylcholine. However, the precurarisation with rocuronium had no statistically significant effect on the enzyme and, hence, proved ineffective in reducing it after succinylcholine administration. Our results were in consistence with earlier studies.18-20
Conclusion
Pretreatment with rocuronium effectively reduces succinylcholine-induced myoglobin and CK elevations. Since the intervals of 1 minute and 4 minutes between the rocuronium and succinylcholine administrations have the same effect on enzyme levels, for busy operating lists, an interval of 1 min appears to be a more time-saving technique compared with an interval of 4 minutes.
Acknowledgements
We would like to thank the Anaesthesia Department at the Combined Military Hospital, Rawalpindi, and the laboratory staff at AFIP.
References
1. Ikram M, Ishaque M, Masood N. Pretreatment with lignocaine; effects on pain of rocuronium injection and withdrawal movement of the arm. Prof Med J Dec 2010; 17: 633-7.
2. Abbas N, Tariq S, Khanzada AA.To assess the effects of rocuronium pretreatment on succinylcholine induced fasiculations and postoperative myalgias. J Pak Med Assoc 2009; 59: 847-50.
3. Schreiber JU, Lysakowski C, Fuchs-Buder T, Tramèr MR. Prevention of succinylcholine-induced fasciculation and myalgia: a meta-analysis of randomized trials.Anesthesiol 2005; 103: 877-84.
4. Wong SF, Chung F. Succinylcholine-associated postoperative myalgia. Anaesthesia 2000; 55: 144-52.
5. Yousef MA, Vaida S, Somri M, Mogilner J, Lanir A, Tamir A. Changes in creatine phosphokinase (CK) concentrations after minor and major surgeries in children. Br J Anaesth 2006; 96: 786-9.
6. Turan A, Mendoza ML, Gupta S, You J, Gottlieb A, Chu W, Saager L, et al. Consequences of succinylcholine administration to patients using statins. Anesthesiol 2011; 115: 28-35.
7. William K. Mallon, Samuel M, Ron M. Rocuronium vs succinylcholine in the emergency department. J Em Med 2009; 37: 183-8.
8. Farhat K, Waheed A, Bakhtiar S, Pasha AK. Comparative study of succinylcholine and precurarization with rocuronium on muscular effects in patients undergoing surgery under anaesthesia. Pak J Pharmacol 2012; 28: 33-41.
9. Sorensen MK, Bretlau C, Gatke AM. Rapid sequence induction and intubation with rocuronium-sugammadex compared with succinylcholine: a randomized trial. Br J Anesth 2012; 108: 682-9.
10. Naoko Fukano N, Takahiro Suzuki T, Kiyoko Ishikawa K. A randomized trial to identify optimal precurarizing dose of rocuronium to avoid precurarization-induced neuromuscular block. J Anesthesia 2011; 25: 200-4.
11. Findlay GP, Spittal MJ. Rocuronium pretreatment reduce suxamethonium induced myalgia: comparison with rocuronium. Br J Anesth 1996; 76: 526-9.
12. Abraham V, Kumar AR, Afzal L. Evaluation of Post Succinylcholine Myalgia and Intubation Conditions with Rocuronium Pretreatment: A Comparison with Vecuronium. Clinical Investigation 2008; 52: 551.
13. Aaron F. Kopman, Nabeel AK, Neuman GG. Precurarization and Priming: A Theoretical Analysis of Safety and Timing. Anaesthesia Analgesia 2001; 9: 1253-6.
14. Marsch SC, Steiner L, Bucher E. Succinylcholine versus rocuronium for rapid sequence intubation in intensive care, a prospective, randomized controlled trial. Critical Care 2011; 15: 199.
15. Appiah J, Ankam MJ, Hunter JM. Pharmacology of neuromuscularblocking drugs. Contin Educ Anaesth Crit Care Pain 2004; 4: 2-7.
16. Kudoh I, Sakai A, Ishihara TG, Matsuki A. Increase in serum creatine phosphokinase after succinylcholine during sevoflurane or isoflurane anaesthesia in children. Br J Anaesth 1997; 78: 372-4.
17. Lorenz D, Stark E, Richter A. Laproscopic hernioplasy versus conventional hernioplasty, results of a prospective randomized trials. World J Surg 2000; 24: 739-46.
18. Martin R, Carrier J, Pirlet M, Claprood Y. Rocuronium is the best non-depolarizing relaxant to prevent succinylcholine fasiculations and myalgia. Can J Anaesth 1998; 45: 521-5.
19. Ozlu O, Mert A. Effects of rocuronium pretreatment on muscle enzyme levels following suxamethonium. Paediatr Anaesth 2002; 12: 151-5.
20. Fatemeh H, Mojgan R. Comparison of atracurium and "mini-dose" succinylcholine for preventing succinylcholine-induced muscle fasiculations: a randomized, double-blind, placebo-controlled study.Acta Anaesthesiol Taiwan 2010; 48: 28-32.
21. Wong SF, Chung F. Succinylcholine-associated postoperative myalgia. Anaesthesia 2000; 2: 144- 52.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: