
Huma Qureshi ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi-35. )
Najmuddin Banatwala ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi-35. )
Sarwar J. Zuberi ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi-35. )
S. Ejaz Alam ( PMRC Research Centre, Jinnah Postgraduate Medical Centre, Karachi-35. )
February 1988, Volume 38, Issue 2
Original Article
Abstract
Emergency endoscopy was done in 306 patients with acute upper gastrointestinal bleeding. Most of the patients were in the age group 20—39 years. Male to female ratio was 2.3:1. The main causes of bleeding were peptic ulcer (40.1 8%), oesophageal varices (32.4%) and superficial mucosal lesions (13.9%). Causes of bleeding remained obscure in 7.2% cases; dual lesions were seen in 2.94%. Complete follow up was available in 83.8% cases of portal hypertension and 69.10% peptic ulcers. Overall mortality in portal hypertension and peptic ulcer was 42.4% and 13.2%, respectively. Poor correlation was found between clinical and endoscopic diagnosis (JPMA 38 : 30, 1988).
INTRODUCTION
The diagnosis of the cause of upper G.I bleeding is notoriously difficult and there is no substitute to actual visualization of the source of bleeding. The value of fibreoptic endoscopy, within 24 hours of upper gastrointestinal bleeding, is well known.1-5 It helps in the diagnosis of acute erosive and superficial mucosal lesions of the oesophagus, stomach and duodenum which are often missed even with double contrast barium studies. The present study was undertaken to determine the various causes of upper G. I. bleeding and compare the accuracy of clinical diagnosis with the endoscopic findings.
MATERIAL AND METHODS
Three hundred and six consecutive patients with a history of haemetemesis or malaena in the previous 24 hours, referred to PMRC Research Centre, were included in the study. The data mostly comprises of the inpatients of Jinnah Postgraduate Medical Centre. Haemetemesis was defined as vomiting of blood, blood clots and/or coffee ground vomitus and malaena as passage of black or dark brown tarry loose stools. Rebleeding was defined as a definite rebleed within 10 days of the last bleeding. The dinicai data, clinical diagnosis, radiological and endoscopic findings were recorded on a standard proforma. Endoscopy was done with Olympus GIF P2 fibreoptic pan endoscope in left lateral position, using 4% xylocaine for topical anaesthesia. No premedication was used for the procedure. The patients were followed till discharge or death.
RESULTS
Age and Sex
The ages of patients ranged between 15 - 90 years (mean 40 years). Majority of the cases were in the age group 2 1 - 39 years (Table 1) with a male: female ratio of 2.3:1 .
Causes of Bleeding
Peptic ulcer (40.18%) was the commonest cause of bleeding, followed, in the descending order of frequency, by oesophageal varices (3235%) and superficial mucosal lesions (SML) (13.9%) like oesophagitis, gastritis and duodenitis. Other lesions (7.11%) included carcinoma of oesophagus, stomach and bleeding vessels. In 7.20% cases the causes of bleeding remained undetermined (Table I).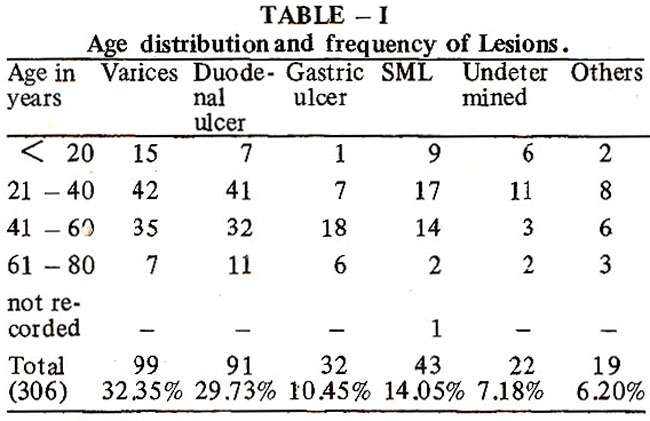
Dual lesions were seen in 294% cases. Of 26 patients with a history of drug ingestion (aspirin, anti-arthritic drugs) only 6 (24%) had superficial mucosal lesions. Frequency of rebleeding was maximum in patients with oesophageal varices (19.1 9%) and duodenal ulcer (17.58%) (Table II).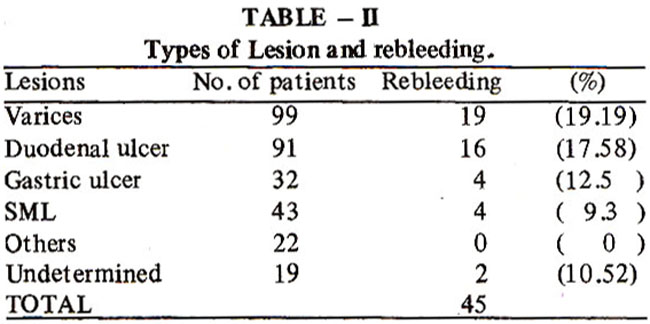
The aetiology of portal hypertension was cirrhosis in 44, idiopathic in 38 and extrahepatic in 3. It remained undetermined in 14 cases. Five patients with bleeding oesophageal varices had dual lesions. During follow up, 20 portal hypertensives underwent surgery (11 non-shunt procedures and 9 shunts). Seven patients died in the immediate post- operative period due to bleeding and two died later. Overall mortality for oesophageal varices was 42.42%, bleeding (79%) being the commonest cause of death followed by hepatic coma (Table III).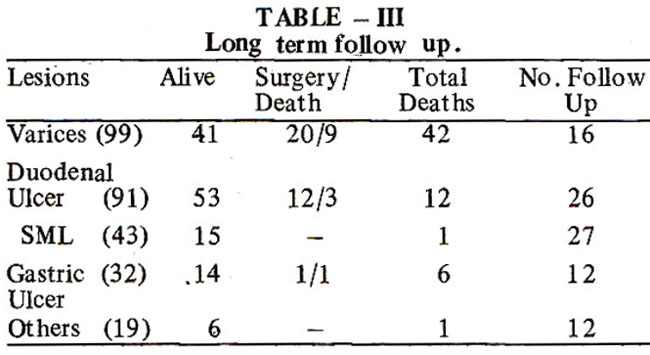
Twelve patients with duodenal ulcer underwent surgery following failure to respond to medical therapy. 0f91 cases with duodenal ulcer, 12 (13.2%) died; nine (75%) died of rebleeding and 3 (25%) after surgery (Table III). In each case, clinical diagnosis was recorded before endoscopy and later compared with the endoscopic diagnosis to see the accuracy rate. Except for a better correlation in oesophageal varices, endoscopic diagnosis was always more accurate than clinical diagnosis (Table IV).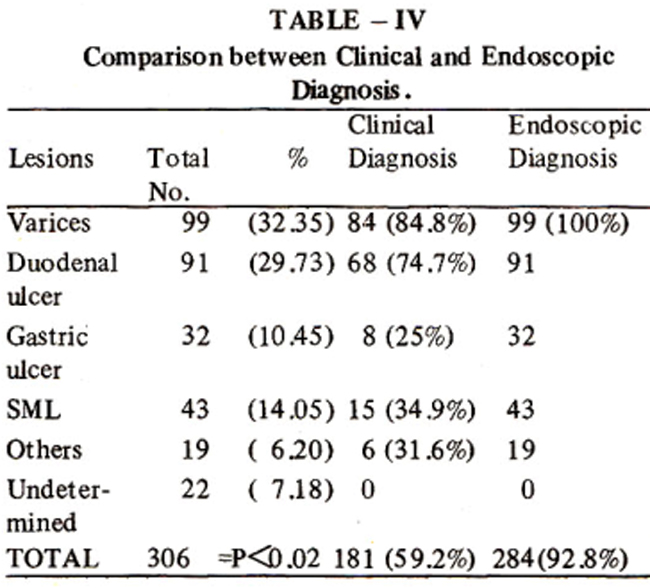
DISCUSSION
Early endoscopy in cases of upper gastrointestinal bleeding has considerably altered the older concepts of the causes of bleeding, but the consequences of the event have remained the same. In the present study, accurate diagnosis of the causes of bleeding was done, within 24 hours of the onset, in about 93% cases. Male predominance (23:1) especially of a younger age group was similar to other reported series5,6, but not as high as that of India (4.7: l) 5. A wide variation, in the frequency of various lesions causing upper gastrointestinal bleeding, was seen in the present study and other reported series3,5-12 (Table V).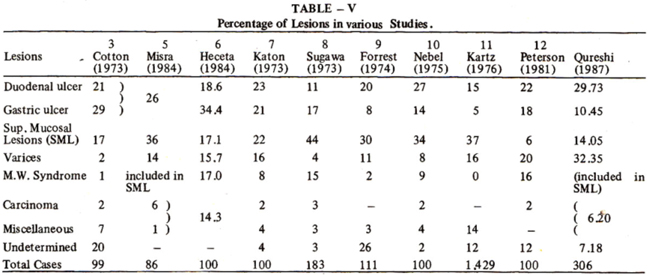
Peptic ulcer disease (40%) remains the commonest cause of bleeding in our patient population, which is very similar to other studies3,6,7,10,12. In contrast, 4 reports (Table V) show acute superficial mucosal lesions as being the more frequent cause of upper gastrointestinal haemorrhage. 5,8,9,11 The results of the present study may be indicative of the dominant frequency of peptic ulcer among all lesions of the upper gut, whether bleeding or not. The preponderance of gastric over duodenal ulcers among bleeders may also, likewise, be a consequence of a higher frequency of gastric ulcer in the population with upper gastrointestinal complaints. Gastric ulcer was 3 times less frequent than duodenal ulcer in this study. Duodenal ulcer was the second commonest cause of rebleeding and death in the present study. Stigmata of bleeding (bleeding vessel, clot) were present in small number of cases but they had no correlation with the frequency of rebleeding. It is therefore suggested that duodenal ulcer patients with a previous history of bleeding should be warned for rebleeding and kept in follow up. Old patients living in the far flung areas should be offered surgery in order to reduce the frequency of rebleeding and death. Unlike other studies, variceal bleeding in cases of cbrhosis of liver and idiopathic portal hypertension was the second most common cause of upper G.l. bleeding. In studies like this where superficial mucosal lesions are infrequent, the presence of non-bleeding varices and other lesions can be taken as the cause of bleeding. Superficial mucosal lesions are recognized as a frequent cause of bleeding in studies where emergency endoscopy is done to determine the cause of bleeding. Their frequency varies from 6-44%.12,8 Conversely, in large series where endoscopy was not done, their frequency went down to 2% or less. 13-16 Superficial mucosal lesions were not a major cause of bleeding in the present study. Mention must be made of the poor correlation between clinical and endoscopic diagnosis, which was also reported by others. 17-19 The value of early upper gastrointestinal endoscopy in ascertaining the cause of bleeding is well recognised by all those who use this procedure. The present experience of 306 consecutive upper gastrointestinal endoscopies in bleeders was associated with a high yield of the bleeding lesion. The procedure, being a diagnostic one, cannot influence the resulting morbidity and mortality, but the valuable information obtained from it makes it an important tool for the diagnosis and management of upper gastrointestinal bleeding.
ARNOWLEDGEMENT
Referral of patients by the professorial and resident staff of intensive care unit and medical unit II, JPMC and secretarial help of Mr. Riaz Hussain is gratefully acknowledged.
REFERENCES
1. Allen, H.M. , Block, M.A. and Schuman, B.M. Gastroduodenal endoscopy management of acute upper gastrointestinal haemorrhage. Arch. Surg., 1973; 106 :450.
2. Machado, G., Scussel, P,J.and Salmon, P.R. 3rd world Congress of gastrointestinal endoscopy Mexico city, in topics in gastroenterology, part 3. Oxford Blackwell, l975,p. 20.
3. Cotton, P.B., Rosenberg, M.T. and Waldram, R.P.L. Early endoscopy of a esophagus, stomach and duodenal bulb in patients with haemetemesis andmelaena. Br. Med. 3., 1973; 2:505.
4. Hoare, A.M. Comparative study between endoscopy and radiology in acute upper gastrointestinal haemorrhage. Br. Med. J., 1975; 1:27.
5. Misra, R.C., Tewari, A., Jam, S.K., Dewan, R. and Minotra, S.K. Cinico-endoscopic correlation in patients with upper gastrointestinal bleeding. Indian 3. Gastroenterol., 1984; 3: 211.
6. Hecta, E.G., Domingo, E.O. and Gloria, V.I., Makalinao All and Limson, A. Upper gut pànendoscopy in upper Gastrointestinal Haemorrhage. Phil.J.Int.Med., 1984;22:87.
7. Katon, R.M. and Smith, F.W. Panendoscopy in the early diagnosis of acute upper gastrointestinal bleeding. Gastroenterology, 1973; 65 : 728.
8. Sugawa, C., Werner, M.H., Hayes, D.F., Lucas, C.E. and Walt, AJ. Early endoscopy; a guide to therapy for acute haemorrhage in the upper gastrointestinal tract. Arch. Sing., 1973; 107:133
9. Forrest, J.A.M., Finlayson, N.D.C. and Shearman, D.1.C. Endoscopy in gastrointestinal bleeding. Lancet, 1974;2 :394.
10. Nebel, O.T., Fornes, ME, Macionus, R.F. et al. Duodenoscopy inthe diagnosis of upper gastrointestinal bleeding. Milit. Med., 1975; 140:110.
11. Kartz, D., Pitchumoni, CS., Thomas, E. and Antonelic, M. The endoscopic diagnosis of upper gastrointestinal haemorrhage. Changing concepts of etiology and management. Dig. Dis., 1976; 21:182.
12. Peterson, W.L., Barnett, C.C., Smith,H.J. ,Allen, M.H. and Corbett, B.D. Routine early endoscopy in upper-gastrointestinal-tract bleeding; a randornized, controlled trial. N. Engl. 5. Med., 1981 ;304:925.
13. Berko witz, D., Thompson, C.M.,Sussman, I. and Gambescia, J.M. Acute upper gastrointestinal haemorrhage a rational approach to diagnosis and management. JAMA., 1956; 160 : 1398.
14. Warthin, TA., Ross, F.P., Baker, D.V.Jr. and Wissing, E. The management of upper gastrointestinal haemorrhage. Ann. Intern. Med., 1953; 39 :241.
15. Zimmerman, S.L., Engel, E.F., Lapidus, B., Bradley, E.A. and Claytor, H. An analysis of 200 admissions for massive upper gastrointestinal bleeding. Ann. Intern. Med., 1956; 45: 653.
16. Atik, M. and Simeone, F.A. Massive gastrointestinal bleeding ; study of two hundred ninety six patients at city Hospital of Cleveland. Arch. Sing., 1954;69: 355.
17. Katz, D., Friedman, E. and Selesnick, S. Endoscopy in acute upper gastrointestinal bleeding. Am. J. Dig. Dis., 1958; 3: 734.
18. Palmer, E.D. and Brick, I.B. Sources of upper gastrointestinal haemorrhage in cirrhotic patients with oesophageal varices. N. Engl. J. Med., 1953; 248 :1057.
19. Dagradi, A.E. , Sanders, D. and Stempien, S.J. The sources of upper gastrointestinal bleeding in liver cirrhosis. Ann. Intern. Med., 1955;42 :852.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: