
S. Hafiz ( Department of Microbiology, The Aga Khan University Hospital, Karachi. )
P. Hamedanit ( Departments of Medicine, The Aga Khan University Hospital, Karachi. )
N. Lyall ( Department of Microbiology, The Aga Khan University Hospital, Karachi. )
J.Ali ( Liaquat National Hospital, Karachi. )
R. Memon ( Charania Hospital, Karachi. )
S. Ali ( Liaquat National Hospital, Karachi. )
Mansoor Ali ( Departments of Medicine, The Aga Khan University Hospital, Karachi. )
M. Ansari ( Department of Microbiology, The Aga Khan University Hospital, Karachi. )
September 1989, Volume 39, Issue 9
Original Article
Abstract
Three hundred random sputum samples were collected for analysis from cases of mild to severe respiratory infections and screened for Legionella pneumophila by both the culture method and also the direct fluorescent antigen test. In one Third of the cases, blood specimen was also collected and screened for Legionella serum antibodies. With the direct fluorescent test it was possible to identify Legionella in 9% of the samples while the culture gave positive results in 4.3% of cases. Diagnostic antibody titers (1:256) were obtained in 12% of the samples while another 12% cases showed serum antibody titers of 1:64 to 1:128. In Pakistan where antibiotics are used extensively, the direct fluo rescent examination of sputum samples gives more accurate diagnosis of Legionella cases than the culture method (JPMA 39: 229, 1989).
INTRODUCTION
Since its first outbreak in 1976 at the American Legion Convention in Philadelphia, Legionellainfeclions have become a common cause of both community acquired and nosocomial cases of pneumonia.1 Legionella pneumophila, the causative agent of Legionnaires disease, has a wide distribution in natural and man made aquatic environments. 2 The common specimens sent for a laboratory diagnosis are sputum, respiratory fluid and tissue. These samples have a high growth yield as compared to blood cultures. Positive cultures in rare cases have been obtained from wound abscesses, prosthetic heart valves and in one case even from a perirectal abscess. 3 In recently infected cases the direct fluorescence test for Legionella antigen and the culture method are useful laboratory diagnostic procedures. Serum antibodies against Legionella start to appear 5-10 days after illness and reach maximum litres in 2-4 weeks. In Pakistan Legionella is not routinely screened by any of the laboratories for economical and technical reasons, as well as due to the lack of awareness. Keeping in view that very few laboratories in Pakistan may be in a position to do only one or maximum 2 of the 3 established methods of Legionella detection i.e. direct fluorescence, culture and serum antibodies, we used all these 3 methods to evaluate their comparative value.
MATERIALS AND METHODS
Specimen: Sputum samples were collected from 300 patients with mild to severe respiratory infections. These were evaluated for the presence ofLegionellapneumophila both by culture and the direct fluorescence method. In 100 out of 300 cases a single blood sample was obtained and screened for Legionella antibodies also.
Culture Media: Oxoids Buffered Charcoal Yeast Extract (BCYE) medium with growth supplement (SR 110) and selective supplement (SR 118) was used for primary isolation. Sub-cultures were made on media without selective supplements. The media were prepared according to the manufacturers instructions. Clinical samples were inoculated on the BCYE medium containing selective agents incubated at35 - 37°C in5% C02 with increased humidity. Plates were checked for growth after 24 hours. Any growth in 24 hours was disregarded. Plates were incubated for 15 days but checked everyday. Any growth after 48 hours was regarded suspicious of Legionella. These colonies were stained by Gram’s method in which safranin was substituted by 0.1% dilute fuchsin. Safranin does not or, weakly, stains the organisms as compared to dilute fuchsin. For confirmation Of isolates, any Gram negative pleomorphic rods seen were checked for oxidase reaction, catalase test and inoculated onto cysteine free medium. Its sensitivity tested against Erythromycin and Tetracycline also made for direct fluorescence staining.
Direct Fluorescent Staining (D.F.):
A smear was made from the clinical spedmens for D.F staining using Genetic systems direct fluorescent kit5 and manufacturer’s instructions were followed. Culture confirmation stained smears were also prepared and were examined under the Olympus fluorescence microscope.
Indirect Fluorescent Antibody litre (I.F.A.T):
I.F.A.T. was performed on serum using Zeus I.F.A.T6 kit according to the manufacturer’s instructions.
RESULTS
Growth on BCYE agar medium appearing after 48 hours was suspected for Legionella. Colonies were emulsified in distilled water for motility test. Grams stain which showed pleomorphic Gram negative organisms varying from coccobadilli to long rods but having a constant width, weekly oxidase positive, motility positive, positive on direct fluorescence and requiring cysteine were confirmed as Legionella. As an indirect confirmation, all these isolates were also found to be sensitive to erythromycin and Tetracyline.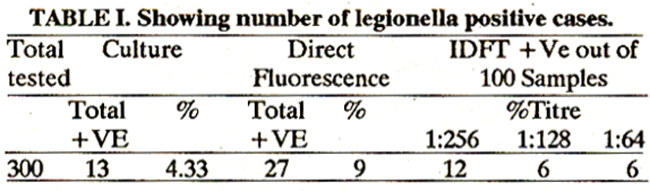
Table summarizes the results of all positive Legionella obtained by the three methods. 9% of samples were positive by direct fluorescence method, while 433% were positive On culture. 24% of the blood samples gave antibody titres ranging from 1:64 to 1:256 but according to the criteria of single diagnostic titre being 1:250 or more, only 12% gave a positive titre.
DISCUSSION
Thouqh culture technique has been reported to be more sensitive for Legionella isolation than the direct fluorescence test, in this study we observed that the direct fluorescence test gave twice as many positive Legionella cases compared with the culture method. Test results with the direct fluorescence test are obtained within 24 hours as compared with the culture method which takes from 3-15 days. In developing countries such as Pakistan, financial constraints make the direct fluorescence test more expensive. Hence it is advisable for local laboratories to atleast initially culture all sputum specimens for Legionella, particularly those from patients with severe chest infections, since 90% of our positive results were from the severely ill pneumonia cases. Our culture results maybe less positive as compared to other studies undertaken in developed countries since the problem of antibiotic abuse is significantly higher in our set up viz a viz that of countries in Europe or in the United States. Also some of our Legionella positive sputum specimens were from tuberculosis patients who had been on antibiotics for upto several months, before these current sputum culture were done. Keeping in view the excessive antibiotic abuse, and other local disease conditions such as tuberculosis, it can be suggested that compared to Western countries a negative Legionella culture cannot be as significant in ruling out Legionnaires disease in developing countries, who have a similar environment to that in Pakistan. With indirect fluorescence method positive serum antibody titres were seen in24% cases ranging 1:64 to 1:256. According to the data from Western countries only 12% had a significant titre of 1:250 which suggested a recent infection in a convalescent patient. 8 76% did not show presence of any antibody in the serum. It is therefore important to assess whether the remaining 12% cases whohad titres of 1:64 or 1:128 had the disease, or were infected currently or had subclinical infection. Before we accept the Western criteria for diagnostic litres it would be worthwhile to do a large survey of a cross section of our population, for the presence of Legionella serum antibodies.
REFERENCES
1. Yu, V.L Nosocomial Legionellosis; current epidemiological issues, in Remington, Swartz, M.N. current clinical topics in infectious disease, 7th ed. McGraw Hill, 239-253.
2. Stout, J.E., Yu, V.L and Best, M.G. Ecology of Legionella pneumophila within water distribution systems. Appl. Environ. Microbiol., 1985; 49:221.
3. Arnow, P.M., Boyko, Li. and Friedman, E.L. Perirectal abscess caused by Legionella Pneumophila and mixed anaerobic bacteria. Ann. Intern. Med., 1983; 98: 184.
4. Weatherall, Di., Ledingham, J.G.G. and Warrell, D.A. ed. Oxford Text Book of Medicine Oxford, Oxford University Press, 1987, p3.
5. Genetic Systems, 3005 First Avenue, Seattle WA 98121.
6. Zeus Scientific Inc., P.O. Box 38, Raritan NJ. 08869.
7. Braunwald, E., Isselbacher, K.J., Petersdorf, RU., Wilson, J.D., Martin, J.B. and Fauci, A.S. Harrisons principles of internal medicine. 11th ed. New York, McGraw Hill, 1987, p. 623.
8. Weatherall, Di., Ledingham, J.G.G. and D.A. ed. Oxford Text Book of Medicine. Oxford, University Press, 1987, p3.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: