
M. Masudul Hasan Nun ( Department of Cardiology, Combined Military Hospital, Rawalpindi. )
June 1989, Volume 39, Issue 6
Original Article
Abstract
From January 1983- December 1986 a total of 880 patients were received by the ‘flying Squad Team’ from Rawalpindi and Islamabad. The average uelay between the onset of chest pain and medical aid was considerably less in those patients evacuated by ‘Flying Squad’ compared to those who cameon theft own (3.2 + 1.2 SEM hours vs 6.5 + 2.0 SEM hours). Eighteen cases developed cardiac arrest outside hospital of which 14(77.8%) were successfully resuscitated. Eleven (61.1%) left the hospital alive. Pre-hospital coronary care is an important adjunct to the hospital coronary care which significently reduces mortality (JPMA 39:157, 1989).
INTRODUCTION
Flying squad services have existed in Rawalpindi/Islamabad for over four years. The need for such services was realised because the clinical picture in the first few hours following onset of myocardial infarction is quite different from that seen in the coronary care unit. Autonomic disturbances which could trigger fatal arrhythmias are much more common and at this stage, the severity of ischaemic damage is most likely to be altered by appropriate emergency treatment1,2. Most fatalities due to ischaemic heart disease occur before a patient reaches hospital and many do not show warning symptoms3 . If patients with symptoms of acute myocardial ischaemia receive medical care within the first hour a significant reduction in mortality could be expected4. Accordingly, to deliver basic life support outside the hospital a rapid response emergency care system named “Hying Squad Service”, was operated at AFIC/NIHD Rawalpindi. The purpose of this report is to review the achievements and drawbacks of the pre-hospital systàm over the last four years (January, 1983 - December, 1986).
MATERIALS
The Flying Squad Ambulance consists of a Defibrillator, portable drug box (consisting of life saving medicines), equipment for intravenous therapy and endotracheal intubation, a Medical Officer - trained in the cardio-pulmonary restscitation, NursingAssistant - also trained in the cardio-pulmonary resuscitation, Stretcher bearer, Ambulance driver and Radiotelephone for consultation with the Cardiologist on call/hospital.
METHODS
Calls for the flying Squad may come either from a patient or medical practitioner. Calls are received by a central control, which notifies the stand-by flying Squad on call in the unit Fart-I Order. Within five minutes the team leaves for the place of call. The activities of the team are periodically reviewed to ensure that they are not treat-lug inappropriately. The Flying Squad team are authorised to administer DC defibrillation, insert intravenous line and give specific drugs for specific indications. If there is doubt about management of some aspect of the patient’s ailment, the medical officer can contact the cardiologist on call or hospital on the radiotelephone for advice.
RESULTS
Between January 1983 and Decembçr 1986 a total of 880 calls were received by the Flying Squad Team. Out of these 840 ‘cases were evacuated to the hospital for advanced medical treatment. This forms 17% of total admissions to the coronary care unit (4860 cases). Seven hundred and fifty calls were received from Rawalpindi and 130 from Islamabad. An average delay of 3.2 ± 1.2 SEM hours was observed in cases brought to the hospital after initial treatment while the duration increased to 6.5 ± 2.0 SEM hours for those cases who came on their own to the hospital.
Of 880 cases received, 757(86%) were coronary cases. Myocardial infarction was the cause in 475(54%) cases and coronary insufficiency in 282 (32%) cases, remaining 123 (14%) were non-coronary cases. The details are given in the Table.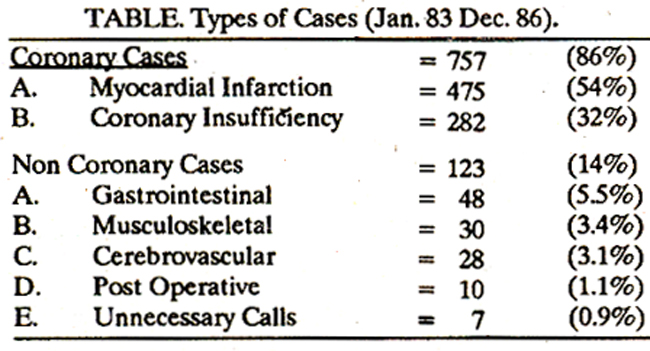
Of 18 cases who developed cardiac arrest outside hospital, 14(77.8%) cases had successful resuscitation, and 4 (22.2%) died. All 110 cases who were brought on their own expired; these cases had cardiac arrest at home or during transit.
DISCUSSION
Mobile coronary care is an integral part of a stratified system for emergency cardiac care and has been developed to bring coronary care to the patient in his home5. The concept introduced by Pantridge in Belfast in 1966 was an advance of great importance6. In 1970 he argued that early treatment of cardiac abnormalities and blood pressure following myocardial infarction might prevent an unnecessary extension of the infarct and this led to the growing interest in the limitation of infarct size7. In the year to follow, other countries also developed such services depending. upon theft requirement and resources8. The flying Squad Service was set up in AFIC/NIHD Rawalpindi in 1982. Two regular fully equipped ambulances started functioning from January 1983. In the present study 86% cases had coronary disease, 54% being myocardial infarction and 32% coronary insufficiency. The remaining cases had non-cardiac problems. In the Pantridge series, 2753 calls were received of whom 43% had proven myocardial infarction and 33% coronary insufficienc9. In 18 cases who were evacuated in our series cardiac arrest occurred outside the hospital. Fourteen (77.8%) out of these were successfully revived and 11 (66.1%) cases left the hospital alive. Of the direct admissions, 110 cases were brought in dead, these cases either developed cardiac arrest at home or during transit. The high mortality reflects lack of basic CPR training amongst attendants and relatives. In Seattle, Washington, during the first three years of operation of Seattle unit, 202 patients were resuscitated6lS% of whom subsequently left the hospital alive10 . In Belfast 193 patients had cardiac arrest outside hospital and resuscitation was attempted in 155. Of these there were 55 initial survivors and 38 left the hospital alive9. In Northern Ireland two comparable areas in a community were surveyed, one bad pre- hospital coronary care and the other hospital coronary care only. Mortality in the area with a mobile unit bad 38% lower values than the other area. This difference was more obvious amongst younger age groups11. Similarly on introduction of a mobile unit, community mortality was substantially reduced amongst persons below the age of 70 in Charlottesville, Virginia12. Results from other studies4 suggest that many lives can be saved by these types of serBasic life support if provided by non-medics can achieve a survival rate of 20%10 and this rate is nearly 40%, if the cardiopulmonary resuscitation is provided by a trained attendant13. If defibrillation is delivered within a short time 50% survival is achieved14. The survival rate increases to 70% if an ideal situation is available with a defibrillator at hand15. Complications of cardiac arrest are minimised when cardiopulmonary resuscitation and defibrillation have been performed in a short time16,17. There is sufficient indication that the quality of life after resuscitation is good in patients who survive and leave hospital18-22. The relatively smaller number of patients requiring cardiopulmonary resuscitation in our series does not under-estimate the usefulness of pre-hospital care. It should be noted that these figures apply to the early years of our service. The delays on the part of patients/doctors requestipg for the service, difficult roads and lanes of Rawalpindi and relatively slow manoeuverability of our ambulances all contribute, though little, to the delays in providing immediate care. It is however, expected that as time goes on considerably better results will be expecte4. For the pre-hospital service to fulfill its role adequately the patients suffering from chest pain must request medical aid as soon as possible. This can only be achieved if the public are aware of the significance of these symptoms. Special emphasis should be placed upon the education of those at high risk23 . Another aspect is instruction in cardiopulmonary resuscitation amongst the public. A large majority who suffer a cardiac arrest do so outside hospital. If a high percentage of the community understood the principles of external cardiac compression and emergency, mouth to mouth ventilation, then there is good chance of the patient being kept alive until Hying Squad Team arrives24,25. The standard depends largely upon the interest and involvement of the medical officer organising and assisting the service. A system of continuing supervision and instruction is essential. In words of one of the pioneers of pre-hospital coronary care Dr. J.S. Geddes “The proficiency of hospital doctors in basic and advanced life support must kee.p pace with the progress being made by citizens and paramedical workers26."
REFERENCES
1. Gordon, T. and Kannel, W.B. Premature mortality fromcoronary heart diseases; The Framingham study. JAMA., 1976; 215:1617.
2. Pantridge, J.F., Webb, S.W., Adgey, A.AJ. and Geddes, IS. The first hour after the onset of acute myocardial in farction, in progress in cardiology. Edited by P.N. Yu and J.F. Goodwin ‘Philadelphia; Lea and Febiger, 1974, p.173.
3. Gillum, RE., Feinleib, M., Margolis, J.R, Fabsitz, RR. and Brasch, RC. Delay in pre hospital phase of acute myocardial infarction. Lack of influence on incidence of sudden death. Arch. intern. Med., 1976; 136:649.
4. Grace, WJ. and Chadbourn, J.A. The first hour in acute myocardial infarction. Heart Lung, 1974; 3:736.
5. American Heart Association. Standards for cardiopulmonary resuscitation (CPR) and emergency cardiac care (ECC). JAMA., 1974; 227(suppl):837.
6. Pantridge, J.F. and Geddes, J.S. A mobile intensive care unit in the management of myocardial infarction. Lancet, 1967; 12:271.
7. Pantridge, J.F. The effect of early therapy on the hospital mortality from acute myocardial infarction. QJ. Med., 1970; 39:621.
8. Pantridge, J.F., Adgey, A.A.J., Geddes, J.S. and Webb, S.W. The acute coronary attack. Tunbridge Wells; Pit-man Medical, 1975, p.130.
9. Adgey, A.A., Allen, J.D., Geddes, J.S. et al. Acute phase of myocardial infarction. Lancet, 1971; 21:501.
10. Cobb, LA., Alvarez, H. III, Medic 1: The Seattle System for the management of out of hospital emergencies, in National Conference of Standards for Cardiopulmonary Resuscitation (CPR) and Emergency Cardiac Care (ECC). Dallas: American Heart Association, 1975,p.179.
11. Methewson, LM., McCloskey, B.G., Evans, A.E., Rus sell, CJ. and Wilson, C. Mobile coronary care and community mortality from myocardial infarction. Lancet, 1985; 1:441.
12. Crampton, RS., Aldrich, RE., Gascho, J.A., Miles, J.R Jr. and Stillerman, B.. Reduction of prehospital, ambulance and community coronary death rates by the community - wide emergency cardiac care system. Am.J. Med., 1975; 58:151.
13. Thomson, RG., HaIlstorm, A.P. and Cobb, LA. By standard initiated cardiopulmonary resuscitation in the management of ventricular fibrillation. Mn. Intern. Med., 1979; 90:737.
14. Cobb, LA. and Hallstorm, A.P. Community-based cardiopulmonary resuscitation; what have we learnt? Mn. N.Y. Acad. Sd., 1982; 382:330.
15. Weaver, W.D., Cobb, L.A., Hailstorm, A.P., Fahrenbruch, C., Copass, M.K. and Ray, R Factors influencing survival after out of hospitat cardiac arrest. J. Am. Coil. Cardiol., 1986; 7:752.
16. Weaver, W.D., Copass, M.K., Bufi, D., Ray, R., HaIlstorm, A.P., and Cobb, LA. Improved neurologic recovery and suçvival after early defibrillation. Circulation, 1984; 69:943.
17. I3ergner, L, Bergner, M., Hailstorm, A.P., Eisenberg, M.S. and Cobb, LA. Service factors and health status of survivors of out of hospital cardiac arrest. Am. £ Emerg. Med., 1983; 1:259.
18. Guzy, P.M., Pearce, M.L and Greenfield, S.The survival benefit of bystander cardiopulmonary resuscitation in a paramedic sewed metropolitan area. Am. 3. Public Health, 1983; 73:766.
19. Eisenberg, M.S., Bergner, L. and Hailstorm, A.P. Paramedic programs and out-of hospitai cardiac arrest. 1. Factors associated with successful resuscitation. Am. J. Public Health, 1979; 69:30.
20. Stults, KR, Brown, D.D., Schug, V.L. and Bean, J.A. Prehospital defibrillation performed by emergency medical technicians in rural communities. N. Engl. J. Med., 1984; 310:219.
21. Mackintosh, A.F., Crabb, M.E., Grainger, it, Williams, J.H. and Chamberlain, D.A. The Brighton resuscitation ambulances; reviewof 40 consecutive survivors of out-of-hospital cardiac arrest. Br. Med. J., 1978; 1:1115.
22. Wennerblom, B., Ekstrom, L. and Holmberg, S. Resuscitation of patients in cardiac arrest outside hospital. Comparison of two different organizations of mobile coronary care in one community. Eur. Heart J., 1984; 5:21.
23. Mandel,LP., Cobb, L.A. CPRtrainingin the community. Ann. Emerg. Med; 1980; 31:453.
24. Vincent, R., Martin, B., Williams, 0., Quinn, B., Robertson, G. and Chamberlain, D.A. A community training scheme in cardio-pulmonaiy resuscitation. Br. Med. J., 1984; 1:617.
25. Cobb, LA., HaIlstorm, A.P., Thompson, R.G., Mandel, L.P. and Copass, M.K Community cardiopulmonary resuscitation. Annu. Rev. Med., 1980; 31:453.
26. Geddes, J.S. Twenty years of prehospital coronary care. Br. Heart 1, 1986; 56:491.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: