
Radar Jehan Farooqui ( Department of Clinical Microbiology, The Aga Khan University Hospital, Karachi. )
Mohammed Khurshid ( Departments of Pathology, The Aga Khan University Hospital, Karachi. )
Mehboob Alam ( Department of Clinical Microbiology, The Aga Khan University Hospital, Karachi. )
May 1989, Volume 39, Issue 5
Original Article
Abstract
Over two years, 9892 mid-stream urine samples from patients attending the Aga Khan University Hospital, Karachi were cultured. Significant bacterial growth was seen in 23.5% samples. Further identification of these organisms Eevealed 40% of E.coli, 16% Pseudomonas aeruginosa, 11% Klebsiella aerogenes, 5.0% Enterobacter sp., 13% Protdus sp., 4.0% Serratia liquifaciens, 1.0% Acinetobacter sp., 3.0% Citrobacter sp., 4.0% Enterococci, 0.5% Staphylococcus aureus. Results of sensitivity tests performed with antibiotics Ampicillin, Cotrimoxa.zole, Nitrofurantoin, Nalidixic acid, Gentamicin, Amikacin, Pipemedic acid, Cefotaxime, Azactain and Carbenicillin did not reveal any distinct pattern (JPMA 39:129,1989).
INTRODUCTION
Urinary tract infection is a commonly observed condition in clinical practice1. Studies show prevalence rate of 1-2% in neonates, mostly boys and upto 2.0% in school girls, some 50 times more than those of boys of similar age. Figures available for pre-school children suggest that it tends to become commoner in girls during infancy2. The prevalence of bacteriuria in adult men is low 0.1 or less until the later years where surveys have shown prevalence of bacteriuria to be about 4-15%3-6. The diagnosis of urinary tract infection cannot be made without bacteriological culture of urine. Patients with classic symptoms of urinary tract infection may have sterile urine and asymptomatic patients may have infected urine. The laboratory diagnosis of a primary urinary tract infection depends upon the demonstration of significant bac teriuria i.e. 1&organisms per ml by quantitative culture of freshly voided sample of urine7-9. The effective management of urinary tract infection needs the knowledge of various organisms and theft sensitivities to antibiotics. The present study was undertaken at The Aga Khan University Hospital, Karachi to provide this data.
MATERIAL AND METHODS
1992 samples of urine were collected randomly, for culture and sensitivity tests, from patients of Medical, Surgical, Paediatric wards and patients attending out-patients departments of The Aga Khan University Hospital and also those referred from other general practitioners in Karachi. Samples coliected in sterile screw capped containers as a mid- stream urine were sent to the Microbiology Laboratory within an hour of collection2,9. Samples which could not be delivered within an hour were refrigerated at 4°C for upto 24 hours10. Each urine sample was mixed well and by using a 5 mm diameter calibrated loop11 was cultured by Cystine Lactose Electrolyte Deficient (CLED) agar plates. Plates were included at 37°C for 24 hours and colony formation units were counted for the presence of bacteria in urine. All significant Gram negative rods were identified by an Anal2ytical Profile Identification (A.P.I. 20E) system12 Antibiotic ‘sensitivities tests were done on diagnostic sensitivity plates (DST) by Stoke’s method13.
RESULTS

Table I shows the commonest bacteria causing urinary tract infection in out-patients is E.coli. Pseudornonas aeruginosa is the commonest cause of urinary tract infection in hospitalized patients. Table II shows resistance pattern of isolates. E.coli, the most common organism isolated showed a high resistance pattern to Ampicillin and Cotrimoxazole 58% and 60% respectively. Generally a higher percentage of the organisms isolated were resistant to Ampicillin and Cotrimoxazole as compared with other antibiotics as shown in Table II.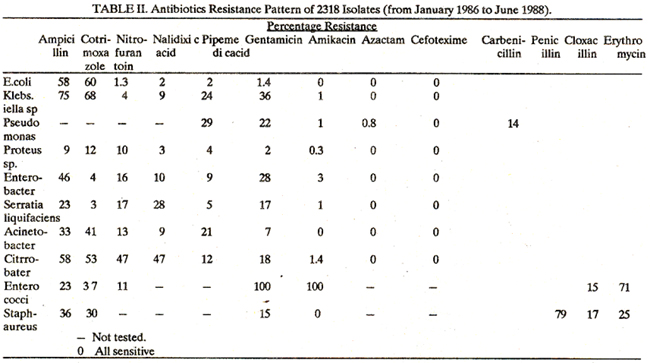
DISCUSSION
The study shows E.coli as the commonest organism causing urinary tract infection. This is in kee3ping with the studies carried out by Ahmad et al13 from Karachi. Studies from West also show £.coli as the most common urinary pathogen15,16. The frequency of other organisms isolated in our study also coincides with Ahmad el al13. However, the resistance patterns of these organisms are different to those reported byAhmad et al13 in 1975 where the most frequent organism E.coli was 62% resistant to Ampidilhin and 13% resistant to Cotrimoxazole, whereas our study shows a similar resistance pattern to Ampicillin and 60% resistance to Cotrimoxazole, an increase in resistance towards Cotrimoxazole from 13% to 60%. The other isolated organisms show a similar pattern to those reported earlier14. Abbas et al16 have also carried out antibiotic sensitivity study in children with urinary tract infection but did not quote any figures. It appears that E.coli is still the commonest pathogen in urinary tract infection and the bacterial spectrum has not changed over the last 10 years. However, due to frequent and perhaps unwarranted use of Cotrimoxazole, resistance has in-creased making it unsuitable as front-line antibiotic in urinary tract infection. The Aga Khan University Hospital’s study points to the need of frequent monitoring of bacterial spectrum in urinary tract infection and their antibiotic sensitivities so that front-line or blind antibiotic therapy could be designed. Based on our current results, we would recommend Nitrofurantom as a drug of choice for the treatment of urinary tract infection and Gentamicin for more serious infections. However, we must stress urinary tract infections should be investigated fully including microbiological cultures and antibiotic sensitivity tests.
REFERENCES
1. Loudon, I.S., and Green halgh, G.P. Urinary tract infection in general practice. Lancet, 1962; 2:1246.
2. White, R.H.R. Urinary tract infection in children. Br. Med. 3., 1977; 1:1650.
3. Kass, E.H., Savage, W., Santamarina, B. The significance of bacteriuria in preventive medicine in: Kass, E.H. (ed): Progress inpyelonepbritis, Philadelphia, Davis 1965; p.3.
4. Freedman, L.R., Phair, J.P., Seki, M. et al. The epidemiology of urinary tract infection in Hiroshima, Yale]. Biol. Med., 1965; 37:262.
5. Sanford, J.P. Urinary Tract Symptoms and Infection. Ann. Rev. Med., 1975; 26:85.
6. Wolfson, S.A., Kalmanson, G.M., Rubini, M.E. and Guze, LB. Epidemiology of bacteriuria in a predominantly geriatric male population. Am. J. Med. Sci., 1965; 250:168.
7. Leigh, D.A. and William,J.D. Methods for the detection of significant bacteriuria in large groups of patients. J. Gin. Pathol., 1964; 17:498.
8. Kass, E.H. Asymptomatic infection of Urinary tract. Trans. Assoc. Am. Physicians, 1956; 69:56.
9. Kass, E.H. Bacteriuria and the diagnosis of infections of the urinary tract. Arch. Intern. Med., 1957; 100:709.
10. Watson, P.G., and Duerden, B.I. Laboratory assessment of physical and chemical methods of preserving urine specimen.]. Gin. !athol., 1977; 30:532.
11. Hoeprich, P. Culture of Urine.]. Lab. Clin. Med., 1960;56:899.
12. Analytical Profile Index API. System S.A. Labalmeles Grottes - 38390 montalieu vercieu..
13. Ahmad, S.I., Zafar, T., Farooqui, S., and Naqvi, S.AJ. Urine examination of 1,460 patients suspected of urinary tract infection. JPMA., 1975; 25:169.
14. Garrod, LP., Shooter, R.A., and Cutwen, M.P. The results of chemotherapy in urinary infections, Br. Med. J., 1954; 2:1003.
15. William, J.D., Thomlinson, J.L, Cole, J.G. and Cope, B. Asytnptomatic urinary infection in gynaecological outpatients. Br. Med.]., 1969; 1:29.
16. Abbass, i.A., Ashiq, B. and Barney, M.I. Bacterium in children. JPMA., 1983; 33:197.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: