
S. Hafiz ( Department of Microbiology, The Aga Khan University Hospital, Karachi. )
N. Lyall ( Department of Microbiology, The Aga Khan University Hospital, Karachi. )
May 1989, Volume 39, Issue 5
Original Article
Abstract
The incidence of urinary tract infection in our community is studied taking into consideration the indiscriminate and inappropriate use of antimicrobial agents and describing a simple method which could be adopted to evaluate samples of urine for the presence of antimicrobial agents. It reveals that 42.9% individuals were actually on antimicrobial agents and had sufficient levels in their urine to inhibit growth of the most common causative agent of urinary tract infection (JPMA 39:126, 1989).
INTRODUCTION
Bacteriuria literally means presence of bacteria in the urine. This constitutes urinary tract infection involving areas ranging from the kidney to the urethra. The probability of the presence of infected urine in the bladder can be ascertained by quantitating numbers of bacteria in voided urine or urine obtained via urethral catheterization. There is a great difference between the bacterial flora of the urine in patients with primary episode of urinary tract infection as compared with the flora of secondary urinary tract infection. In the primary UT!,E. coli is the most frequent infecting organism while in the so called secondary urinary tract infection the relative frequency of infection caused by Proteus, Pseudomonas and Kiebsiella-Enterobacter species and by Enterococci and Staphylococci increase greatly1. Urinary tract infections are more common in females than in males. Once a woman develops infection she is more likely to develop subsequent infections than one who has had no previous infections2. Stamey and Pfan3 reported that females at the child bearing stage, when seen for the first time, presented with symptoms of uncomplicated urinary tract infections due to Eseherichia coil and the strains were usually susceptible to antimicrobial agents including sulfonamides and, as a high degree of correlation exists between urinary sterilization and in vitro susceptibilities, some argue that it is unnecessary to obtain cultures from these patients. However, it is generally accepted that it is essential to obtain urine cultures4. The diagnosis of urinary tract infections cannot be made without the help of a cultural examination of urine and minimal diagnostic criteria5. Significant bacteriuria is a term that has been used to describe the numbers of bacteria in voided urine exceeding the numbers usually due to contamination from the anterior urethra i.e. _ 105 bacteria/mI6. The implication is that the presence of 105 bacteria/mi urine infection must be seriously considered. Several methods can be employed to quantitate bacteria in the urine7. It has become a common practice in our local laboratories to culture urine without assessing whether the patient is on some antibacterial drug or excreting antibacterial agents which may interfere with the culture giving a false negative or insignificant result. We decided to screen the urine samples received in our. laboratory for the presence of antibacterial agents to get a true spectrum of urinary tract pathogens.
MATERIALS AND METHODS
Specimen: 1100 mid-stream urine samples of patients with suspected urinary tract infections received in the laboratory were subjected to routine culture and simultaneously screened for the presence of antibacterial agents. Culture: Urine samples were cultured onto Cystine Lactose electrolyte deficient medium (CLED oxide) using 5 mm ioop and if growth obtained 50 or more colony forming units of a single type it was taken as significant growth giving a count of orgs/ml8. The isolates were identified and confirmed by the methods recommended by ASM Manual of Clinical Microbiology, 1985.
Detection of Antimicrobial Agents:
a) Organism Used: Sensitive strain of Escherichia was used.
b) Media: Oxoid Isosensitest agar was made according to the manufacturer’s instruction and plates were poured giving a depth of 3-4 mm (20 ml in a 8.5 cm petri dish).
c) Blank Discs: Discs measuring 8 mm were made from Whatman No.2 filter paper, sterilized and stored in sterile universal container.
d) Method: Presence of antimicrobial agents in urine was detected by making a lawn with 18-24 hours old broth culture of sensitive E.coli and the turbidity adjusted to give 105 CFU/ml. Blank discs were dipped in urine and placed onto the seeded plate. On one plate upto six urine samples could be tested for the presence of antimicrobial agents. The plates incubated at 37°C for 24 hours and results recorded. Zone of inhibition indicated the presence of antimicrobial agents.
RESULTS
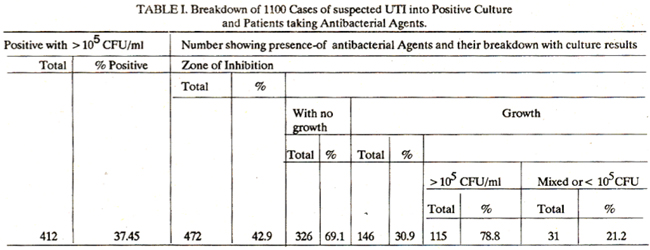
Table I lists the findings of 1100 urine samples, the overall infection rate was 37.45% but it was interesting to note that 42.9% individuals were on antimicrobial agents and among this group only 30.9% showed any growth while in 70% cases urine was sterile.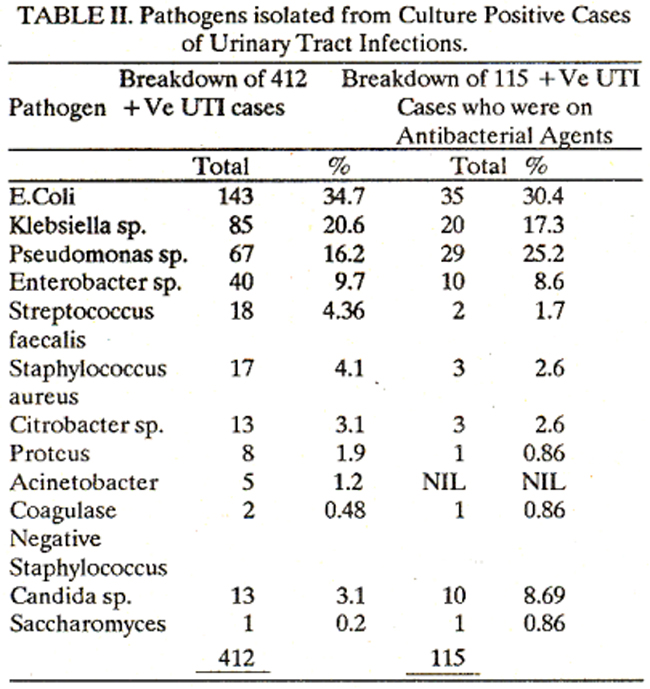
Table II gives the distribution of patients with bacteriuria. E.coli is the commonest cause amounting to 34.7% in all (30.4% in patients on antimicrobial agents) but it is interesting to note that the rate of Pseudomonas infections in patients taking antimicrobial agents is significantly higher while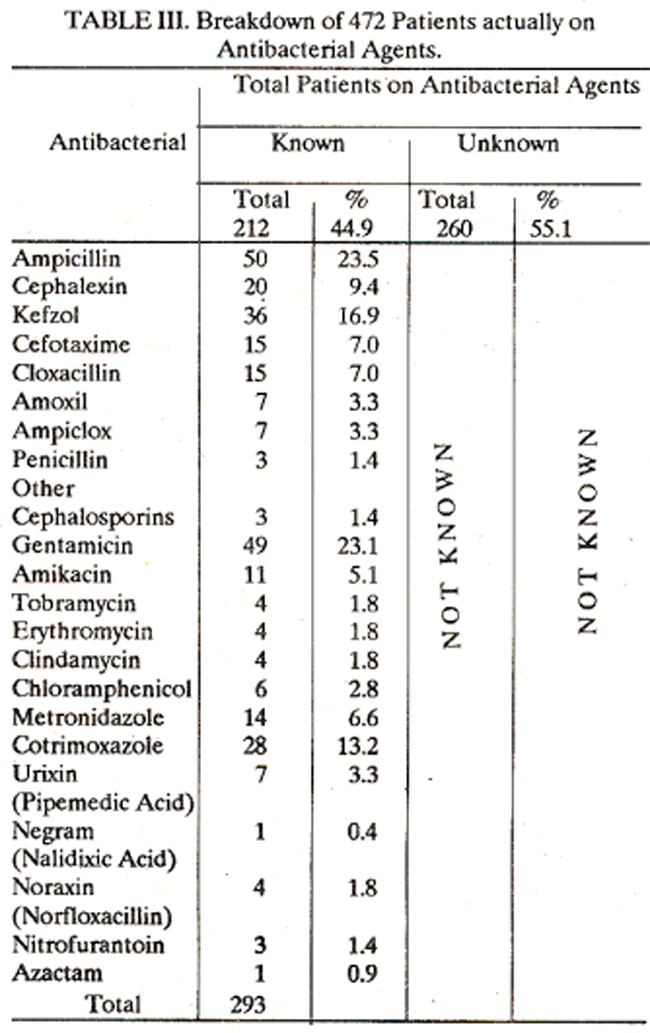
Table III lists the common antimicrobial agents taken by patients prior to collection of sample. More than 50% of patients were on Penicillin and Cephalosporin, 30% on Aminoglycocides and, in all, 38% were taking more than one microbial agents.
DISCUSSION
The study highlights one of the problems assessing urinary tract infections in our country as antibiotics are used as best guess therapy often complicating the prevailing condition and when investigated a false negative insignificant growth obtained resulting in subsequent complications or recurrent urinary tract infections. In episodes where patients experience recurrent bouts of acute frequency and dysuria for which laboratory confirmation of infection was either not sought or was lacking because upto 50 percent of women with such symptoms do not have urinary infection9. It is essential to establish whether or not symptomatic episodes correlates with significant bacteriuriã. A favourable response to “blind” therapy is not a reliable indication that infection is the cause because many attacks of acute frequency and dysuria are self limiting10. In order to have proper investigations done clinicians should refrain from using “blind” therapy and if the patient is taking some antibiotics it should be stopped for atleast 48 hours before submitting a sample as this would enable the laboratories to carry out a more realistic investigation of urinary tract infection. It would not be a bad idea if laboratories carry out a simple test to detect antimicrobial agent in urine and report it if not al ready known. This would be of considerable help to the clinician managing the patient. Even it would be worthwhile to investigate insignificant growth or small numbers (between 10- 10000/ml) of conventional urinary tract pathogens in urine with antimicrobial activity. We are of the opiniOn that the actual rate of urinary tract infections due to common bacterial pathogen in our environment is much higher than what is seen. The overall rate according to this study is 37.45% but if the number of patients on antimicrobial agents is taken into consideration, the true rate would be 47.29%. The overall pattern of bacterial isolates suggests that probably we see more of secondary type of urinary tract infection. One of the reasons for this would be the indiscriminate usage of nephrotoxic antibiotics. Ideally antimicrobial agents should only be administered when there is reasonable evidence of infection in the urinary tract. Symptoms are not a reliable indication of infection6,11. Treatment with an appropriate antimicrobial agent is recommended based on culture report and only one agent should be used; this would ensure effective cure with minimal toxic effects due to blind therapy.
ACKNOWLEDGEMENT
Many thanks to Ms. Fatima Nadir for all her secretarial help in preparation of this manuscript.
REFERENCES
1. Gould, J.C. The comparative bacteriology of acute and chronic urinary tract infection Londonn. Oxford University, 1965.
2. Gillen-water, JX., Harrison, RB., and Kunin, C.M. Natural history of bacteriuria in school girls. A long term case study. N. EngI. J.Med., 1979; 30:396..
3. Stamey, T.A. and Pfan, A. Urinary Infections., a selective review and some observations. Calif. Med. J., 1970; 113:16.
4. Stamey, T.A., Govan, D.E., and Palmer, J.M. The localization and treatment of urinary tract infection;the role of bactericidal urine levels as opposed to serum levels. Medicine, 1965; 44:1.
5. Kunin, C.M. Detection, prevention and management of urinary tract infections. 3rd Ed. Philadelphia Lea and Febiger, 1979.
6. Kass, E.H. Asymptomaticinfection of urinary tract. Trans. Açoc. Am. Physicians, 1956; 69:56.
7. Hoeprich, P. Culture of the urine. J.Lab. Clin. Med., 1960; 56:899.
8. Guttman, D., and Stokes, E.J. Diagnosis of urinaiyinfection; comparison of a pour plate counting method with a routine method. Br. Med. 3., 1963; 1:1384.
9. Mond, N.C., Percival, A., William, J.D. and Brumfit, W. Presentation, diagnosis and treatment of urinaiytract infections in general practice. Lancet, 1965; 1:514.
10. Brumfit,W., Smith, G.W., and Hamilton Miller,J.M. Organization and function of urinary infection clinic part 2. Br. J. Hosp. Med., 1983; 30:381.
11. Gallager, DJ.H., Moptgomerie, J.Z. and North, J.D.K. Acute infections of the urinary tract and the urethral syndrome in general practice. Br. Med. 3., 1965; 1:621.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: