
Naresh K. Panda ( Deptt. of Otolaryngology, Postgraduate Institute of Medical Education & Research, Chandigarh, India. )
Y. N. Mehra ( Deptt. of Otolaryngology, Postgraduate Institute of Medical Education & Research, Chandigarh, India. )
S.B.S. Mann ( Deptt. of Otolaryngology, Postgraduate Institute of Medical Education & Research, Chandigarh, India. )
Satish K. Mehta ( Deptt. of Otolaryngology, Postgraduate Institute of Medical Education & Research, Chandigarh, India. )
May 1991, Volume 41, Issue 5
Original Article
ABSTRACT
A retrospective analysis of 23 cases of post-traumatic facial nerve injury has been done. Majority of the cases had a conductive or a mixed deafness. The Schirmer’s test has been considered to be one of the main indicators to determine the site of injury. The mastoid segment of the facial nerve was found to be injured in 52% of the patients. The surgical approach in patients with post-traumatic facial nerve paralysis should be transmastoid. This can be combined with a middle fossa approach in patients with a positive Schirmer’s test (JPMA 41: 105, 1991).
INTRODUCTION
The management of facial nerve injury resulting from temporal bone trauma continues to be a topic of discussion. The indications for surgery, the timing and extent of surgical exploration are the principal questions debated. The article reviews the authors’ experience in 23 patients of traumatic facial nerve paralysis.
PATIENTS AND METHODS
A retrospective analysis of 23 cases of traumatic facial nerve injury was done at the Nehru Hospital, Postgraduate Institute of Medical Education and Research, Chandigarh, India, during the period between 1985 to 1989. The patients were subjected to electro diagnostic and topographic tests for facial nerve functions in addition to audiologic and radiologic investigations. Only cases of complete facial paralysis with evidence of progressive neural degeneration on nerve excitabifity testing were included. All patients underwent surgical exploration of the facial nerve. Criteria for surgical exploration included a 3.5 milli ampere (MA) or more increase in threshold stimulation over the branches of the paralysed facial nerve compared to the normal side on nerve excitability testing. A transmastoid decompression of facial nerve was done in all cases. Return of facial nerve function was assessed after 6 months of surgical exploration.
RESULTS
Electrodiagnostic
The degree of facial nerve degeneration was determined by the maximal stimulation test in all the cases. Surgery was advised because they had no response or only a barely discernible response to 10 milliamperes on Hilger nerve stimulator.
Audlometric
Ten patients (43.4%) had a conductive hearing loss, 9 (39.1%) a mixed loss, 4 (17.39%) a high frequency sensorineural loss and 3 patients with sensorineural loss were found to have conductive loss on the opposite side.
Topographic: The Schirmer’s test was used as the main indicator to determine the site of facial nerve injury. The result was considered positive, if lacrimation was decreased by atleast 75% on the affected side as compared to the normal side or if lacrimation was less than 10 mm on both the sides, since bilateral reduction in tearing may occur with unilateral greater superficial petrosal nerve injury1. Eleven patients had a positive Schirmer’s test and on exploration, 6 of these patients were found to have injury of facial nerve either in tympanic or mastoid segments. These patients showed either complete (4 cases) or incomplete (2 cases) recovery on follow-up. In the remaining 5 patients, no pathology was seen. The facial nerve was decompressed till the processus cochleari formis in all these cases. The test for the taste of anterior 2/3rd of tongue was positive in 10 out of 23 cases, indicating thereby that the injury was proximal to the origin of chorda tympani. The stapedial reflex was absent in all but one case. This could be due to the presence of conductive loss in the ear under test, which may invalidate the interpretation of the facial nerve function. Of the 10 patients with conductive hearing loss, an ossicular abnormality was encountered in 6 cases. All these patients had a dislocated incus. The ossicular chain in the remaining 4 patients appeared intact but granulations in epitympanum around the ossicular chain of haemotympanum accounted for the impaired conduction. The tympanic portion of the facial nerve was the site of damage in 6 (26%) and the mastoid segment in 12 (52.1%) patients (Figure 1).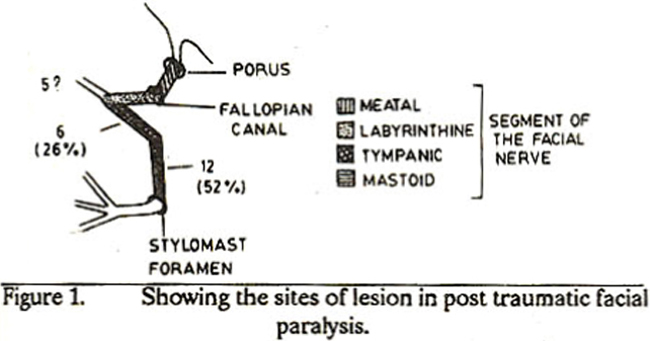
In 5 patients, no pathology was seen either in tympanic or mastoid segments, but the Schirmer's test was positive. It was presumed that there could be injury at or proximal to the geniculateganglion in these 5 patients. Three of these patients had a moderate sensorineural loss on audiometric testing indicating a transverse fracture of the temporal bone. The most commonly observed injury to the facial nerve was an impingement of bony spicules into the nerve sheath from a fracture of the fallopian canal (12 cases). Six patients had evidence of oedema of the nerve alone alongwith inflammation and granulations.
Results of Surgery
Return of facial function was judged according to the following parameters.
Normal
Complete symmetry of the face at rest and for various facial positions including raised eye brows-tight eye closure, wrinided nose, whistling and smiling.
Good
Facial symmetry at rest with only minimal weakness of synkinesis. Mild facial asymmetry and moderate facial weakness with synkinesis.
Poor
Marked facial asymmetry at rest and only minimal return of facial movement. Of the 15 patients, who came for follow-up and evaluation 6 months after surgery, the functional results were normal in 7, good in 6 and fair in 2.
DISCUSSION
Facial paralysis is a more obvious and distressing sequelae of temporal bone trauma. The decision to decompress the facial nerve is based on results of nerve excitability testing. In those cases, where there was no response with 10 mA stimulation, a decision to explore the facial nerve was taken. The tympanic portion, the area of the second genu and the labyrinthine segment of the facial nerve have all been implicated as the common site of lesion. Ney1 in study on the cadavers noted that tympanic portion of the facial nerve is the commonest site involved. Mchugh2 observed that the most common site of injury to the facial nerve in longitudinal and transverse fractures of the temporal bone is within the middle ear. Lambert and Brackmann3 in their series of 26 patients with longitudinal temporal bone fractures found the perigeniculate region to be involved in 80% cases. The injury in their cases was typically located just at the junction of the geniculate ganglion and tympanic portion of the facial nerve. Fisch4 in 28 surgically verified facial nerve lesions found that in 93% of patients, the pathology was in the labyrinthine segment of the facial nerve. In only 7% patients, the lesion occurred between the tympanic and mastoid segments. He suggested that the earlier surgical observations concerning the most common site of injury to the facial nerve in longitudinal fractures5 should be re-evaluated. In our series of 23 cases, the site of facial nerve injury is in contrast to that suggested by Brackmann et al3 and Fisch4. The most common site of lesion was in the mastoid segment (12 cases). The tympanic segment was the site of injury in 6 patients only. The site of injury in our series could probably be due to the mode of injury. The road traffic accidents we encounter mostly involve the two wheelers6. The rider often falls on the side thereby injuring the temporal bone and hence the facial nerve in the vertical portion or the tympanic segment (Figure 2).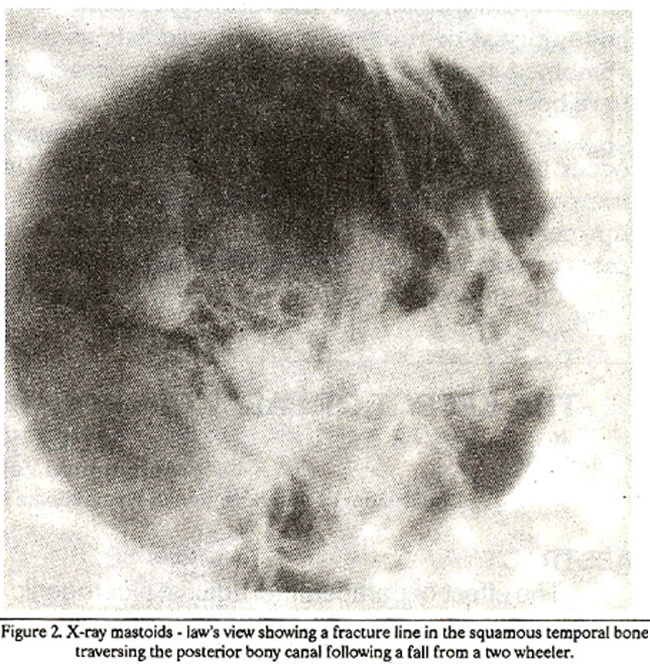
Surgical treatment
Fisch4 advocated middle cranial fossa approach in more than 90% of longitudinal fractures. Brackmann et al3 found that in some cases, the transmastoid extra labyrinthine subtemporal approach can be used. Yanagihara7 had proposed a transmastoid exploration of the temporal bone. Coker et al8 in their arguments against this approach explained many shortcomings in exploring the nerve proximal to the cochleariform process. They suggested that the fracture line in tegmen tympany, bone fragments and granulation tissue hamper dissection of the facial nerve. The exploration of the labyrinthine segment into the internal auditory meatus is unlikely without injury to the superior ampulla and repair is difficult for transections when they occur. Topographic testing is useful in determination of surgical approach to the injured segment of the nerve. A positive Schirmers test would indicate an injury around the perigeniculate ganglion region though false positive results could occur. In our series, the false positive rate of the Schirmers test was 6/11. These patients were found to have injury in either tympanic (2 patients) or mastoid (4 patients) segments and on follow-up after 6 months, had either incomplete or complete recovery. Lambert and Brackmann3 in their series used transmastoid approach for exploration of the tympanic and mastoid segments. A combined transmastoid middle fossa approach was resorted to in-patients with a positive Schirmers test. The rationale for a transmastoid exploration in these cases is since about 20% of patients in their series had double injury. In our series the other 5 patients with a positive Schirmers test where no pathology was encountered either in the tympanic or mastoid segments, could have had injury at or proximal to the geniculate ganglion. A combined transmastoid middle fossa approach could have been useful in these patients. A mild high frequency sensorineural loss, may also occur in a longitudinal temporal bone fracture. Unlike transverse fractures, a longitudinal fracture do not violate the membranous labyrinth. High frequency loss in these cases can occur due to concussive injury to the cochlea. Our findings are in concurrence with Houghs and Stuarts9 report that separation of the incudo stapedial joint is the commonest ossicular injury. Tympano-plastic procedures like incus transposition can be performed after the facial nerve decompression9. The optimal timing for surgical exploration is a matter of discussion. Surgery should be done as soon as the electro-diagnostic tests indicate severe injury and predict a poor prognosis. An immediate facial paralysis followed by a slow progression of degeneration will have a good prognosis, whereas a delayed paralysis with a rapid onset of degeneration should be treated by surgery in order to ensure good recovery.
REFERENCES
1. Ney, K.W. Facial paralysis and the surgical repair of the facial nerve. Laryngoscope, 1922;32: 27.
2 McHugh, H.E. The surgical treatment of facial paralysis and traumatic conductive deaf. ness in fractures of the temporal bone. Ann. Otol., 1959; 68:855.
3. Lambert, P.R. and Brackrnann, D.E. Facial paralysis in longitudinal temporal bone fractures; a review of 26 cases. Laryngoscope, 1984; 94: 1022
4. Fisch, U. Facial paralysis in fractures of the petrous bone. Laryngoscope, 1974; 84: 2141.
5. Mchugh, HE. Facial paralysis in birth injury and skull fractures. Arch. Otolaryngol., 1963;78: 443.
6. Pandhi, S.C., Mehra, Y.N., Golbar, S.V., Masooda and Dewan, LI. Postmortum temporal bone changes in head injury. Indian J. Otolaryngol., 1981; 33: 135.
7. Yanagihars, N. Transmastoid decompression of the facial nerve in temporal bone fracture. Otolaryng, Head Neck Surg., 1982; 90: 616.
8. Coker, N.J.. Kendall, K.A., Jenkins, H.A. and Alford, B. R. Traumatic intratemporal facial nerve injury; management rationale for preservation of function. Otolaryng Head Neck Surg., 1987; 97: 262.
9. Hough, J.V. and Stuart, W.D. Middle ear injuries in skull trauma. Laryngoscope, 1968; 78: 899.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: