
Syed Shershah ( Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. )
John J. Morrison ( Addenbrookes Hospital, Hills Road, Cambridge, England. )
Sadiqa Jafarey ( Department of Obstetrics and Gynaecology, Jinnah Postgraduate Medical Centre, Karachi. )
May 1991, Volume 41, Issue 5
Original Article
ABSTRACT
The prevalence of premenstrual syndrome (PMS) was determined in 1600 women belonging to various socioeconomic groups in Karachi. Of the total, 33% had PMS, whose prevalence was high in lower socioeconomic group living in socially deprived areas. A direct association of PMS was noted with parity, being low in low parity group. Major complaints were pain in lower abdomen, cramps and backache with majority taking no treatment for their complaints (JPMA 41: 101, 1991).
INTRODUCTION
Premenstrual syndrome is a recognised clinical entity since the ancient Greek Hippocrates blamed the agitated blood for shivering, lassitude and heaviness of the head. They explained how the agitated blood found its way to the uterus where it escaped the body causing the relief of symptoms1,2. Frank3 described the typical symptomatology with tension, unrest, irritability, fatigue, lack of concentration, pain and swelling and noted its relationship with the menstrual cycle. A global study suggested premenstrual syndrome as a civilized western phenomenon unlike dysmenorrhoea and menstrual mood changes which is universal4. Most studies1,5-7 show a 30-60% prevalence of PMS, with only 10- 15% cases labelled as severe which require treatment8. The risk factors for PMS include genetic composition, age, parity, alcohol and profession9-13. The diagnosis of PMS is difficult and different methods are designed for its diagnosis in busy gynaecological clinic2,14. As no single drug has been proven effective in the treatment of PMS16, therefore, its management includes education, reassurance and drug therapy. This study was carried out in Karachi to detect the prevalence of PMS in our population.
PATIENTS AND METHODS
One thousand six hundred women from different ethnic and socioeconomic groups filled in a questionnaire in which they noted the presence or absence area of symptoms prior to the menstruation. A woman Shah Paiaal Colony was considered to have Malir Old and New premenstrual syndrome Old Karachi. she had more than three D.H.5. Oifton, symptoms for the last six PECHS, Bb. Abad. months, in each cycle, Nazimabad, N.N.Abad which always occurred Miacellaneous prior to menstruation and Total disappeared with the onset of the period. The PMS . P~ - menstrual Syndrome Soc. Economic group age of menarche, cycle length and duration of menstruation were also noted. Socioeconomic status was evaluated according to the number of family members and their total income. The profession of women and educational status of the family were also noted. The questionnaires were filled in with the help of lady school teachers, and final year medical students (1988 -89) from Dow and Sind Medical Colleges, Karachi.
RESULTS
One thousand six hundred women (1,198 married, 402 unmarried) completed the questionnaires. The total prevalence of PMS was 33.3% with slightly higher frequencyin married (33.6%), than in unmarried women (32.0%). In the married group, PMS related to parity (Table I).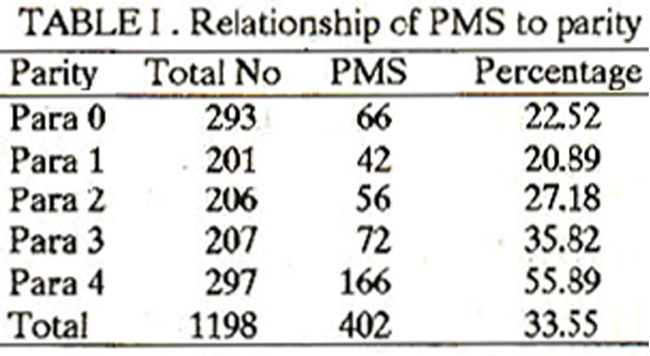
The prevalence was lower in Para 0,1 and 2 while it was higher in Para 3,4 and onwards.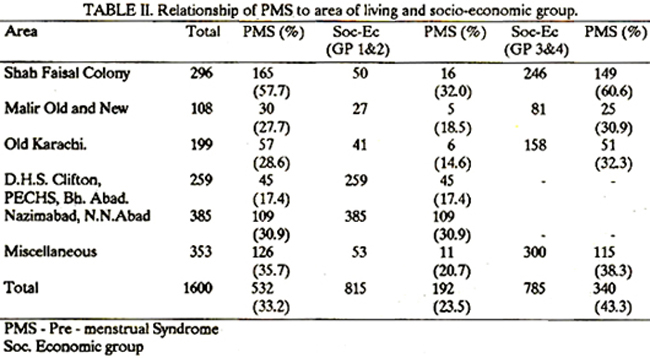
Table II shows the relationship between the area of living and socioeconomic status. The frequency was higher (43.3%) in lower, and low (23.5%) in the higher socioeconomic groups. The highest frequency of PMS (57.7%) was noted is Shah Faisal Colony in both groups of social classes. It was 60.6% in the lower socioeconomic and 32.0% in the higher socioeconomic group. In this particular area the law and order situation has deteriorated over the past few years. Relationship of PMS to the ethnic origin showed that PMS was more frequent in Punjabi and Mohajir population (37% each). A frequency of 30.0% was noted in Sindhi and Baluchi population and a low frequency of 11.6% was recorded in Pathans from Baluchistan and North West Frontier province living in Karachi.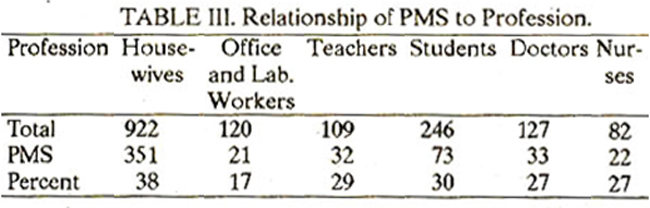
Table III shows the incidence of PMS in various professional groups. PMS was high in housewives (38.0%) and low in office workers (17.5%). Majority of women took no treatment for PMS. Females who went for treatment were treated for dysmenorrhoea with analgesics and vitamins.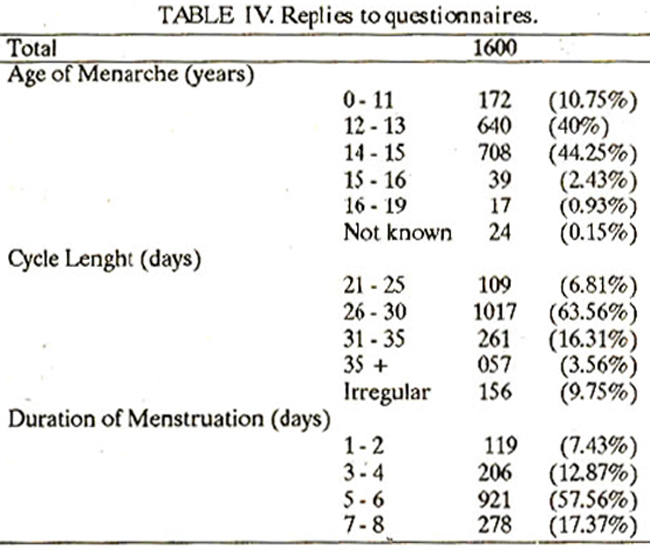
Table IV shows thatmajority of girls (72%) bad their menarche between 12 and 14 years, 9.7% had irregular cycles with duration of menstruation varying between 1-11 days. The data regarding menstrual symptoms suggested that the majority of women had lower abdominal pain (100%), cramps (92%) and backache (88%) (Table V).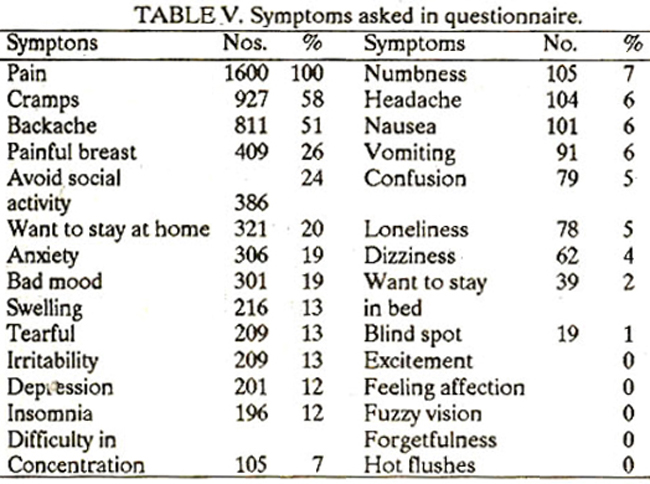
DISCUSSION
There is a need to discuss the population and methods used in this study to understand its limitation before interpreting the result. Karachi is a cosmopolitan city. A big group of the population belongs to those who had migrated from India in 1947 (Mohajir) after independence. Another group consists of immigrants from Bangladesh. Besides, people from rural areas and all provinces keep on pouring into Karachi for better job opportunities. It is a multicultural and multilinguistic society exposed to recurrent obituaries, unrest, law breaking, and persistent tense atmosphere. The population in this study does not represent the majority of the women living in rural areas of Pakistan with different social, educational and cultural backgrounds. The survey was carried with the help of volunteers comprising of medical students, junior hospital doctors, nurses and lady school teachers. The questionnaires were explained to respondents and how they should interpret the questions. It is possible that the explanation and answers were biased because of the knowledge of the volunteers regarding PMS. After considering these limitations our data indicates that PMS is not a western problem only14,16 but a group of women in the Pakistani population also have a complex set of premenstrual changes as are well documented in western women. Its incidence is higher in lower socioeconomic groups and inversely proportional to the number of pregnancies. Our data indicated that the frequency was higher in a population where law and order had deteriorated and the people were living under long term curfew orders. It would be interesting to know the effects of curfew and social unrest on the age of menarche, menopause, fertility and the menstrual cycle pattern. A multi-centre trial is needed to confirm these factors. Our data also indicated that treatment by analgesics, vitamins, hakeems (traditional treatment with herbs) and by hoemeopathic drugs, relieved symptoms in a minor group of women, This is probably a well known placebo effect and there is a need of long term review of these treatments in our population. Our data shows that Pakistani women do experience premenstrual syndrome. There is a need to develop methods to conduct multicentre trial in rural and urban areas to find out the exact prevalence of the disease. There is a need to recognize the syndrome and create awareness regarding its assessment, diagnosis and treatment among medical students and general practitioners.
ACKNOWLEDGEMENT
The authors wish to thank all volunteers who carried out this study with hard work and enthusiasm. Special thanks to Mr. RE. Robinson who allowed me to use all facilities in Addenbrooks Hospital during my stay in Cambridge.
REFERENCES
1. Bickers, W. and Woods, M. Premenstrual tension-Rational treatment Tex. Rep. Biol. Med., 1951; 9: 406.
2. Magos, A. snd Studd, 3. The premenstrual syndrome. Frog, Obstet. Gynaecol., 1984; 5: 334,
3. Frank, R.T. The hormonal cause of premenstrual tension. Arch. Neurol.Psychistry, 1931; 26: 1053.
4. Snowden, It and Christian, B. Patterns and perceptions of menstruation. New York, St Martins Press, p. 113.
5. Woods, N.F., Most, A. and Dey, O.K. Prevalence of premenstrusisymptoms. Am. J. Public Health, 1982; 721: 1257.
6. Rees, L. The premenstrual syndrome snd its treatment. Br. Med. J., 1953; 1: 1014.
7. Sutherlsnd, H. and Stewart, I. A critical analysis of premenstrual syndrome. Lancet, 1965;1: 118ft
8. Johnson, SR. The epidemiology and social impact of premenstrusi symptoms. Clin. Obstet. Gynsecol., 1987; 30: 367.
9. Dalton, K., Dalton, M.E. and Guthrie, K. Incidence of the premenstrual syndrome in twins. Br. Med. 3., 1987; 295: 1027.
10. Abraham, G.E. and Hsrgove, J.T. The incidence of premenstrual tension ins gynaecologi cal clinic. J. Reprod. Med., 1982; 27: 721.
11. Dalton, K. The premenstrual syndrome and progesterone therapy. 2nd ed. London, 1984.
12. Halliday, A., Bush, B. and Cleary, P. Alcohol abuse inwomen aeekinggynaecological care. Obstet. Gynsecol., 1986; 68: 322.
13. Adenaike, O.C. and Abidoye, R.0. Study of the incidence of the premenstrual syndrome in a group of Nigerian women. Public Health, 1987; 101: 49.
14. Hammarback, Stefen. The premenstrual syndrome. Acts Obstct. Gynaeeol. Scand. Supple., 1989; 61: 79.
15. Lurie Ssmual and Berenstein, It The premenstrual syndrome. Obstet. Gynsecol. Surv.,45: 220.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: