
Zafar Nazir ( Department of Surgery, The Aga Khan University Hospital, Karachi. )
Jamsheer Talati ( Department of Surgery, The Aga Khan University Hospital, Karachi. )
July 1992, Volume 42, Issue 7
Original Article
The term angiomyolipoma of the kidney was first introduced by Morgan et al1 to denote an uncommon type of renal tumour with the histological components of thick-walled vessels, smooth muscle cells extending outwards from the vessels in a peritheliomatous fashion and fat cells of the adult and foetal types. Although the tumour is referred to as a renal hamartoma2, a mass containing tissues normally present in the organ but abnormal in their arrangement, in fact, renal angiomyolipoma (HAML) are choriostomas, as the fat is not the normal component of the human kidney3. Isolated angiomyolipomas are relatively rase renal tumours. Till 1988 only 250 cases were reported in English literature. The present study adds 3 additional cases and review the outstanding clinical features and advances in the diagnosis and management. Case 1. L.M.N. a 47 year old diabetic, hypertensive female presented in the outpatient clinic for evaluation for right sided flank pain of 5 months duration. There was no history of bowel or urinary symptoms. Examination revealed a tender, firm and smooth mass measuring approximately 20x15 cm occupying the right side of the abdomen. CBC, urine analysis, 24 hour urinary VMA and biochemical profile were normal. The abdominal ultrasonography and intravenous urography revealed a space occupying lesion in right kidney and fullness of the pelvicalyceal system. The CAT scan revealed a 9 cm nonhomogeneous mass with areas of low attenuation values (-65 hounsfields units) in the right kidney (Figure 1).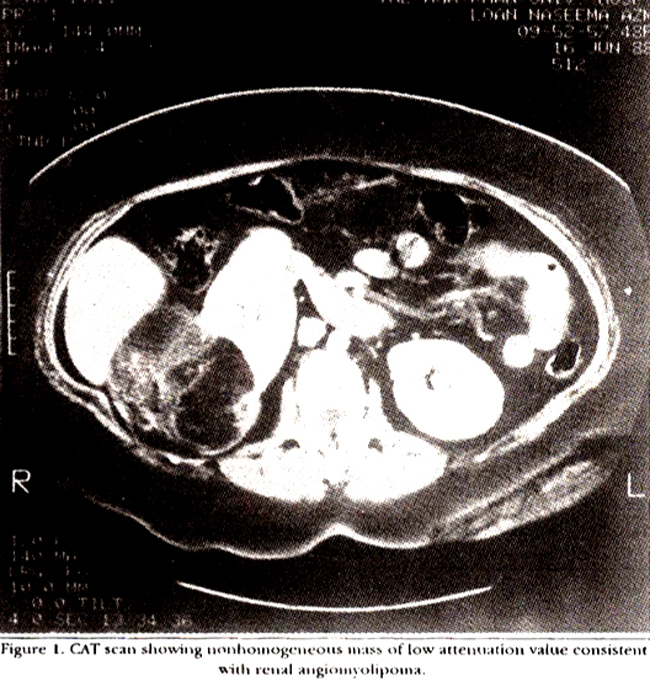
In addition a 2.5 cm solid mass arising from the right adrenal gland was noted. There was no evidence of retroperitoneal lymphadenopathy. Renal cell carcinoma could not be excluded on CT scan appearances. At exploratory laparotomy after opening the gerota’s fascia a tumour mass was seen which was mostly extrarenal but was growing into the right kidney, leaving only a thin rim of cortex. It was soft and spongy to feel and was not vascular. A separate adrenal mass hard in consistency could also be felt. The tumour mass, right kidney and adrenal gland were excised in toto. Histopathology confirmed angiornyolipoma of kidney and adrenal gland. The postoperative course was uneventful and the patient has remained well and symptom free throughout a two years follow- up. Case 2. S.F.N. a 45 year, hypertensive female presented with left lumber pain of one year duration. Her symptoms had worsened since the past month and had become associated with generalized weakness, anorexia, nausea and vomiting. There was no history of fever and urinary symptoms. Examination revealed pallor and a bimanually palpable mass measuring approximately 30x20 cm in left lumber region. Hemoglobin was 9.2 grn/dl with hcmatocrit 27.7%. A urinalysis and routine biochemical profile was normal. An intravenous pyelogram revealed an enlarged left kidney with adequate excretion of dye. An ultrasound (US) of the abdomen showed ahyperechoic mass arising from lateral aspect of left kidney. CT scan of abdomen showed a perinephric hematoma and an intrarenal mass measuring 6x6cm, showing decreased attenuation values (-60 hounsfield units) supportive of fat in the kidney. A renal angiography demonstrated a nonvascular mass, multisaculated aneurysmal dilatation of peripheral artery, sunburst appearance of veins and lack of arteriovenous shunting (Figure 2).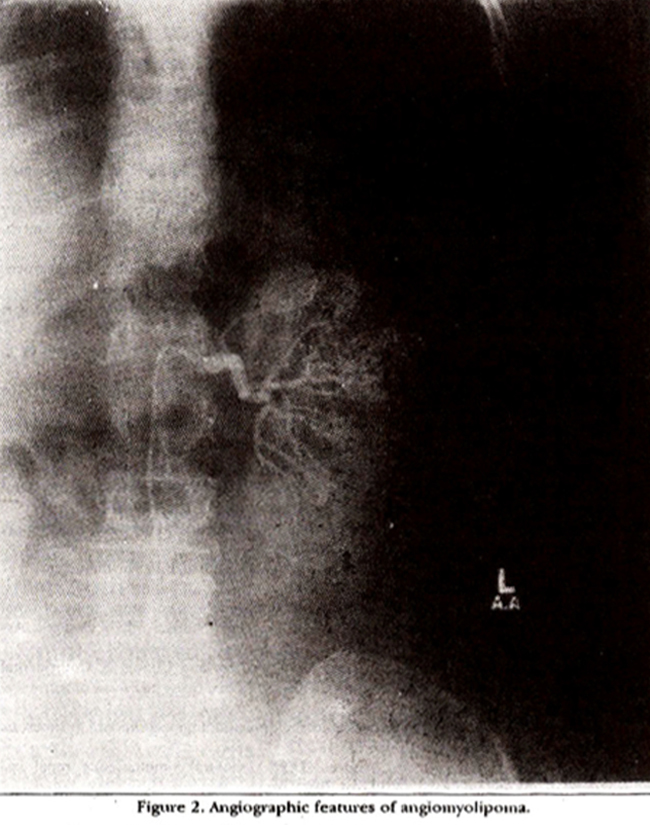
A preoperative diagnosis of RAML was made. Exploratory laparotomy revealed a large perirenal hematoma contained by the gerota’s fascia. Evacuation of hematoma revealed a 6x6 cm, well demarcated, yellowish firm mass arising from the lateral aspect of upper pole of left kidney. Hemostasis was secured by multiple suture ligation and the cavity was obliterated with an omental pedicle. The diagnosis of RAML was confirmed on frozen section and again on final histopathological examination (Figure 3).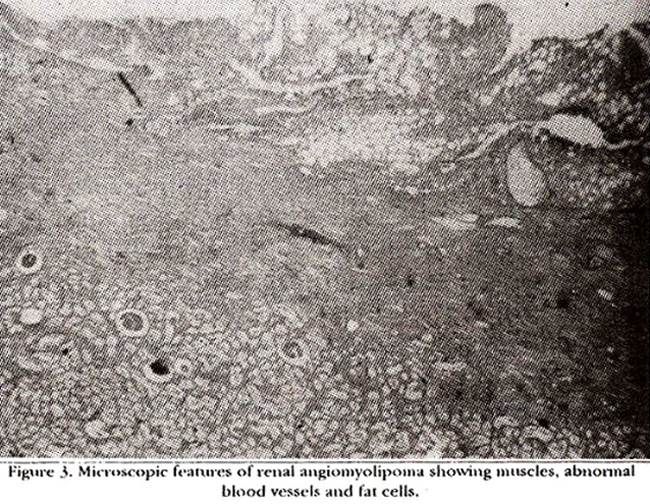
Postoperative recovery was uneventful. The patient has remained symptom free throughout the 18 months follow-up. Case 3. K.A. 34 year old female who was previously in good health presented to the emergency room with acute flank pain associated with nausea, vomiting and sweating. There were no urinary or bowel symptoms. Examination revealed a tender, firm mass measuring approximately 15x10 cm occupying the right side of abdomen. Hemoglobin was 5.1 gm/dl with hematocrit 16.8%. Urinalysis revealed microscopic hematuria. Biochemical profile was normal. Intravenous pyelogram and ultrasound of abdomen revealed a space occupying lesion in the right kidney. CT scan showed perircnal haematoma, a 4 cm smooth mass in the right kidney and a huge retroperitoneal mass with low attenuation value (-65 negative hounsfield units) consistent with diagnosis of RAM!.. The patient normally a resident of London, returned there where she underwent a right nephrectomy. Histopathology revealed RAML.
DISCUSSION
BAML are uncommon benign lesions that may occur as an isolated phenomenon or as seen in 20-50% of patients as part of the syndrome associated with tuberous sclerosis (Bournvill’s disease4). About 50-80% of patients with tuberous sclerosis will have angiomyolipoma5. Therefore these patients require periodic screening as these can be occasionally symptomatic6. RAML as an isolated phenomenon usually present as a large symptomatic unilateral mass. They occur predominantly in women in fifth and seventh decades7. Grossly RAML are greyish-yellow in colour and have propensity for profuse hemorrhage and local aggressive growth7. They may occasionally parasitize to external blood vessels and lymph nodes. The actual incidence of nodal involvement is not known. A review of literature reveals only 8 cases9. The involvement of regional lymph nodes and blood vessels has been attributed to the multicentric origin of the lesion rather than metastatic bchaviour10-13. Todate there has been no death due to mctastatic spread. Microscopically angiomyolipoma consists of sheaths of smooth muscles, abnormal thick wall blood vessels and clusters of adipocytes in varying proportions and arrangements (Figure 3). Renal cell carcinoma may coexist with angiomyolipoma in the same kidney. Twelve such cases until 1989 have been reported in literature9,14,15. One case of simultaneous RAML and oncocytoma has also been reported16. The clinical presentation varies. Symptoms may be absent if the lesion is small (<4cm). When present. symptoms are usually a result of intrarenal or perirenal hemorrhage. More than 50% of patients with angiomyolipomas larger than 4cm have associated hemorrhage12. The most frequent signs and symptoms are acute flank/abdominal pain, palpable mass, hcmaturia, shock and anaemia. Hypertension and fever has been reported8,12. The diagnosis of angiomyolipoma should be borne in mind since 25% of patients with RAML described in the literature presented with severe abdominal pain with or without shock, which necessitated emergency laparotomy8. In the past, correct preoperative diagnosis has been extremely difficult with the result that most patients undergo nephrectomy for a mistaken diagnosis of renal cell carcinoma1,3,12. In recent years CT scan and ultrasonography have resolved the diagnostic dilemma, making definitive diagnosis of RAML possible in almost all cases8,13. Angiomyolipomas are the most echogenic form of renal tumours, due to their high fat content4. However this pattern is not always pathogonomonic since other echogenic lesions, including renal cell carcinoma incorporating perirenal fat, liposarcoma, lipoma, teratoma, oncocytoma, cavernous hemangioma and renal sinus lipomatosis may also exhibit a similar picture. A CT diagnosis of angiomyolipoma requires identification of fat component in the tumour which usually stands out in the lesion as areas with low attenuation value (negative hounsfield unit). Lesions smaller than 2.0 cm may be difficult to diagnose owing to partial volume effect. Moreover a hemorrhage within or outside the tumour may increase the attenuation value to above that of fat17. A 50-78% diagnostic accuracy of CT scan has been reported1,3,8,12,13,17. We were able to make tentative preoperative diagnosis in all of our cases with CT scan but were reluctant to confidently exclude carcinoma except in the case who had angiography (case No.2). Sincc CT scan cannot consistently diagnose all EAML, a fine needle aspiration biopsy (FNA) has been advocated by Scant and associates18 to solve the diagnostic dilemma18. Selective renal angiográphy has been suggested both for diagnostic and therapeutic purposes12. The angiographic characteristic of an angiomyolipoma are hypovascular mass with circumferential tortuous dilated peripheral vessels having multiple aneurysms, sunburst or whorled appearance of the veins and lack of the arteriovenous shunting which is seen in renal cell carcinomas19-21. Selective arterial embolization has been shown to be effective in treating acute hemorrhage alone or in conjunction with surgical intervention4. With accurate preoperative diagnosis of the angiomyolipoma, most urologists currently recommend a conservative approach to the management. The nephrectomy rate has declined from 93% in 1976 to 50% in 198412. For small (< 4cm) asymptomatic tumours, surveillance is all that is required. With large (>4cm) and symptomatic angiomyolipomas, renal conservation with tumour excision or partial nephrectomy are preferred if possible1,3,4,7,8,12. However it is important that conservation should never compromise completeness. Frozen section may be helpful for the diagnosis of coexistent renal cell carcinoma12. In conclusion, renal angiomyolipoma, although a rare lesion, should be included in the differential diagnosis, when dealing with a patient presenting with severe flank pain and anaemia. Considering the benign nature of disease and improvement in preoperative diagnosis, a kidney conserving operation is desirable.
ACKNOWLEDGEMENTS
We wish to thank Dr. Hizbullah Sheikh, Pathology Department, The Aga Khan University Hospital for providing the pathological material and Mr. Muradali Bana for secretarial help.
REFERENCES
1. Tong. Y.C., Chieng. P.U., Tsai. T.C. el at. Renal angiomyolipoma. Report of 24 cases. Br.J.Urol., 1990;66:586-89.
2. Case records of the Massachusetts General Hospital (Case No.51. 1985). N.Engl.J.Med.. 1985;313:1596-1603.
3. Ahmed, I.. Multi, A.B.. Sebayel, M.l. et al. Renal angiomyolipoma. Report of two cases and reviewof literature. Em.Med.J., 1989;7:100-104.
4. Johnson. D.E.,Swanson, D.A. and Eschenbach, A.C.V.Tumoursofthegenitourinary tract, in Smith’s general urology. Edited by K.A. Tanagho and j.W. McAnirch. connecticut, Prentice-Hall, 1988, p.334.
5. Stillwell, T.J.. Gomez, M.R. and Kelalis, PP. Renal lesions in tuberous sclerosis. J.Urol., 1987;138:477-81.
6. Hendren, W.G. and Monfort, Gi. Symptomatic bilateral renal angiomyolipoma in a child. J.Urol., 1987;137:256-57.
7. Dekernion, J.B. Renal tumours, in Campbell\\\'s urology. Edited by P.C. Walsh et al Philadelphia. Saunders, 1986, vol.2, pp. 1294-1342.
8. Blute, ML, Mulek, R.S. and Segura, 3W. Angiomyolipoma: Clinical metamorphosis and concepts for management. J.Urol.,1988; 139:20-24.
9. Taylor, R.S., Joseph, D.B., Kohat, E.C., Wilson, ER. and Bueschen, AJ. Renal angiomyolipoma associated with lymph node involvement and renal cell carcinoma in patients with tuberous sclerosis. J.Urol., 1984;14 1:930-32.
10. McIntosh, G.S., Dutoit, H., Chronos. N.y. and Kaisary, A.V. Multiple unilateral angiomyolipomas with regional lymphangiomyomatosis. J.Urol.,1989;142: 1305.7.
11. Castillenti, J.A. and Bertin, A.?. Angiomyolipoma of the spermatic cord. Case report and literature review. J.Urol., 1989;142:1308-9.
12. Oesterling. J.E.. Fishman. K.E., Goldman, SM. and Marshall. F.F. The management of renal angiomyolipoma. J.Urol., 1986; 135:1121-4.
13. Rothenberg. D.M., Brandt, T.D. and- D\\\'Cruz, I. Computerized tomography of renal angiomyolipoma presenting as right strial mass. J. Compact.Assist.Tomogr.,1986;10: 1054.56.
14. Huang. J., Ho D.M., Wang. .1., Chou, Y., Chen, M. and Chang, S. Coincidental angiomyolipoma and renal cell carcinoma ‘Report of one case and review of literature. J.Urol.. l98$;140 l516-18
15. Graves, N. and Barnes, W.F. Renal cell carcinoma and angiomyolipoma in tuberous sclerosis: Case report. J.Urol., 1986;135: 122-23.
16. Waters, DJ.. Holt, S.A. and Andres, D.F. Unilateral simultaneous renal angiomyolipoma and oncocytoma. J.Urol., 1986;135:568-70
17. Bosniak. M.A., Megibow. A.J., Hulnick, D.H.. Horii. S. and Raghavendra, B.N. CT diagnosis of renal angiomyolipoma: the importance of detecting small amount of fat. AJR., 1988;151:497-501. -
18. Sant, G.R.. Ayers. D.K., Bankoff, M.S., Mitcheson. H.D. and Crei, A.A.Jr. Fine needle aspiration biopsyin thediagnosisof renal angiomyolipoma. J.Urol., 1990;143:999-1001.
19. Peary, N.M., Webb. J.A.W., White, FE. - and Whitfield. H.N. Hemorrhagic angiomyolipoma of the kidney. J.Urol., 1984;132:749. 51.
20. Davis, T.J. Parasitic arterial supply to renal angiomyólipoma. J.Urol., 1978;118:271-74
21. Barzilai, T.M., Braden, G.L., Ford, L.D., Goodman, LH., Delima, R.J.. Germain, M.J. and Fitzglhbons. J.P. Renal angiomyolipoma with arteriovenous shunting. J.Urol., 1987;137:4838-4.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: