
Mohammad Younus Sheikh ( Department of Radiology, The Aga Khan University Medical Centre, Karachi. )
Imtiaz Hussain Rizvi ( Departments of Radiology, The Aga Khan University Medical Centre, Karachi. )
Iftikhar Ahmed ( Departments of Radiology, The Aga Khan University Medical Centre, Karachi. )
June 1992, Volume 43, Issue 6
Case Reports
INTRODUCTION
Number of food stuffs and other oesophageal pathologies have been implicated to carcinoma of the oesophagus but to the best of our knowledge, no relation to Commercially available betel nuts has been described. We present a case of a young female developing carcinoma of the oesophagus which may be due to excessive use of commercially available sweetened betel nuts (raseeli supari).
CASE REPORT
A 30 year old lady presented with history of dysphagia. She gave history of taking 8-10 packets of commercially available betel nuts (raseeli supari) every day for last 10-12 years. Oesophagogram was performed which demonstrated an area of irregular narrowing and shouldering involving lower third of the oesophagus (Figure).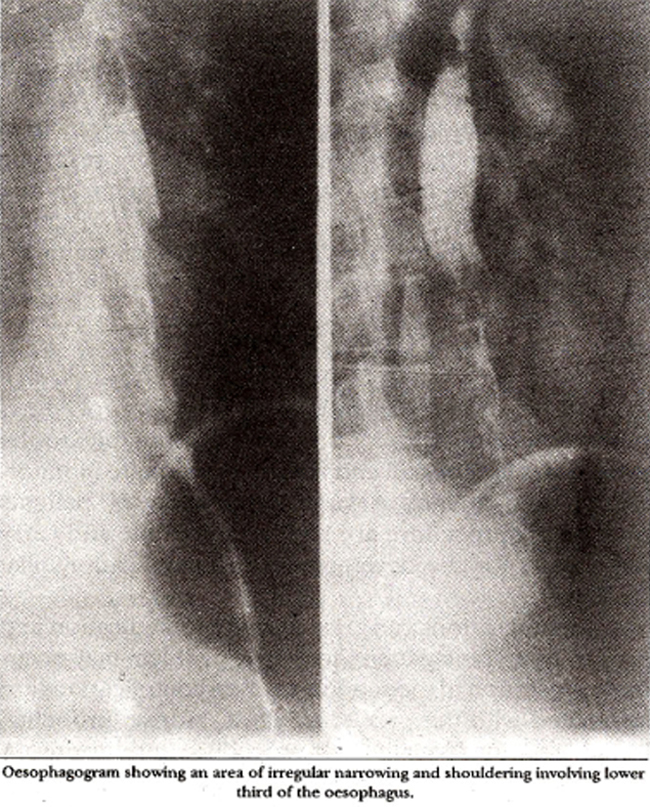
Biopsy of the lesion proved it to be poorly differentiated squamous cell carcinoma. Lesion was thought to be inoperable and after palliative surgery patient was referred for radiotherapy. She expired 9 months after the diagnosis.
DISCUSSION
The evidence on the aetiology of the carcinoma of the oesophagus is largely indirect, based on epidemiological studies and circumstantial inference derived from other coexisting oesophageal pathologies. Carcinoma of the oesophagus is largely a disease of middle aged males; incidence being four times higher in males. Blacks are affected more commonly by the disease1. Different etiological factors have been implicated in different parts of the world, for example in Iran and China carcinoma of the oesophagus is probably due to deficiency of different nutrients like vitamin A, riboflavin, thiamine and pyridoxine and minerals like zinc and molybdenum1-3. Ingestion of hot beverages, coarse food stuffs and presence of nitrates in the food have also been implicated in the causation of chronic oesophagitis which is thought to be precancerous2. In Saudi Arabia water contamination by petroleum, containing benzene and polycyclic hydrocarbons have been postulated to be the causative factor4. German workers exposed to ethylene oxide showed increased incidence of oesophageal carcinoma5 while in Sweden chimney sweeps exposed to polycycic aromatic hydrocarbons had an increased incidence of oesophageal carcinoma6. Dietary habits like consumption of alcohol and smoking1,7,8 are also associated with this disease. Burnt and unburnt tobacco contains nitrosonornicotine which is thought to be the offender carcinogen. Fungal contamination of the food is also carcinogenic7,8. Different oesophageal pathologies have been associated with cancer. These include achalasia1,7,8 oesophageal webs in Plummer Vinson Syndrome7, Zenkér’s diverticulum1,8 strictures caused by Lye ingestion7,8 and hiatus hernia leading to Barrett’s oesophagus8,9. An interesting association between some skin disorders: and oesophageal carcinoma has been noted. These include epidermal dysplasia like tylosis and epidermolysis bullosa1,7. Long standing celiac disease is also associated with the disease. In our case there appears to be a very strong association between oesophageai cancer ancl ingestion of large amount of commercially available sweetene4 betel nut (raseeli supari). As the patient did not belong to the susceptible age group and sex, betel nut is the most likely etiologic agent. The question whether the carcinogen is betel nut itself or artificial sweeteners and colouring agents, needs to be evaluated.
REFERENCES
1. Dayal, Y arid DeLellis, R.A. The gastrointe stinal tract, in pathological basi s of diseases. By Rarnzi S. Cotran, Vinay Kumar and Stanley L Robbins. 4th ed. Philadelphia. Saunders, 1989. pp. 835-36
2. Munoz, N., Crespi, M., Grassi, A., Qing, W.G., Qiong. S. and Cai, L.Z. Precursor lesions ofoesophageal cancerin high-risk populations in Iran and China. Lances, 1982;1:816-79.
3. Noetzel, C., Mobarhan, S., Negal, P., Layden, T. and Junigk, A. Vitamin A and riboflavin nutriture in patients with oesophagial cancer, oesophagesl disorders, psthophysiology and therapy. Edited by T.R. DeMeester and 0.8. Skinner. New York, Raven Press, 1985, pp.319-26.
4. Amer, MM., el-Yazigi, A., Hannan, MA. and Mohammed, M.E. Contamination and oesophageal cancer of Qasim region. Saudi Arabia. Gastroenterology, 1990;98:1141-47.
5. Klesselbach, N., Him, K., Lange, H.J. and Korallus, U. A multicentre mortality atudyof workers exposed to ethylene oxide. Br.J. Industrial Med., 1990;47:182-88.
6. Gustavsson, P., Gustavsaon, A. and Hogstedt, C. Excess of cancer in Swedish chimney sweeps. Br.). Industrial Med., 1988;45:777-81.
7. Moertel, CC. Alimentary tract, in cancer medicine. Edited by James F. Holland, Emil Frel. Philadelphia, Lea and Febiger, 1982, pp.1753-54.
8. Enterline, H.T. and Thompson, J.J. The oeaophagus, in principles and practice of surgical pathology. Edited by Seven C. Silverberg. New York, Wiley, 1983, pp. 805-6.
9. Cooper, B.T. and Barbezat CO. Barrette’s oeaophagus: a clinical study of 52 patients. Q.J. Med., 1987;62:97-108.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: