
Ijaz Ahmed ( Departments of Surgery, King Edward Medical College, Lahore. )
I.D. Qureshi ( Departments of Pathology, King Edward Medical College, Lahore. )
June 1992, Volume 43, Issue 6
Case Reports
Neuroblastomas are the commonest malignant retroperitoneal tumours in infancy and early childhood with a peak incidence at the age of two years1. Their occurrence declines sharply after this age though on rare occasions neuroblastomas have been reported above the age of 152. Neuroblastomas arise from the adrenal medulla and paravertebral sympathetic chain. Very rarely they have been reported as primary tumours of the kidney and are described as pathological curiosity3,4. A case report follows in which a neuroblastoma was encountered as a primary renal tumour in a 21 year old female. This tumour is unusual at this age.
CASE REPORT
A 21 year old female was admitted to the East Surgical Ward with the history of gradually increasing dull pain in the right loin without urinary symptoms for the last one year. She also complained of moderate anorexia, constipation and gradually increasing weakness over this period and lost about 5 Kgs of weight. Two months before admission she developed acute pain in the right iliac fossa and underwent appendicectomy in November, 1989. About six weeks ago she noticed a lump in the right upper abdomen accompanied by occasional bouts of vomiting. Examination revealed an oval non-tender mass in the right hypochondrium which was bimanually palpable. Routine blood and urine investigations were normal. Ultrasonography showed an enlarged right kidney with irregular outer border and poor corticomedullary contrast. A poorly defined solid mass was present in the upper pole and parenchymal echos were disturbed in rest of the area. Renal pelvis was dilated in lower half while deposits were present in the upper half. Left kidney was normal. Intravenous urography revealed a normally functioning left kidney but no excretion of dye on the right side. X-ray chest was clear. With the provisional diagnosis of a renal neoplasm, nephrectomy was carried out through a right paramedian incision. The right supra-renal gland was present above the tumour and was removed alongwith it. it appeared morphologically normal and could be separated from the tumour mass without difficulty. There was no evidence of secondary deposits on the peritoneal surface, in the liver or paraaortic lymph nodes. Postoperative course was uneventful and the patient was sent home on the 8th postoperative day.
Pathological features
The kidney after clearing the perinepbric fat weighted 320 grams. Its capsular surface was smooth and pale pink colour. It had a brownish 4 cm diameter rounded mass in subcapsular region replacing the upper pole. In addition similar smaller patches were seen in the remainingkidney. All these masses and nodules were firm in consistency. Cut section of the specimen was mostly replaced by tumour mass which was pale, lobulated and homogenous with a few areas of haemorrhages. It was transversed by fine fibrous trabaculae. Only a portion of the renal parenchyma was present at the upper pole. No other remarkable features were observed (Figure).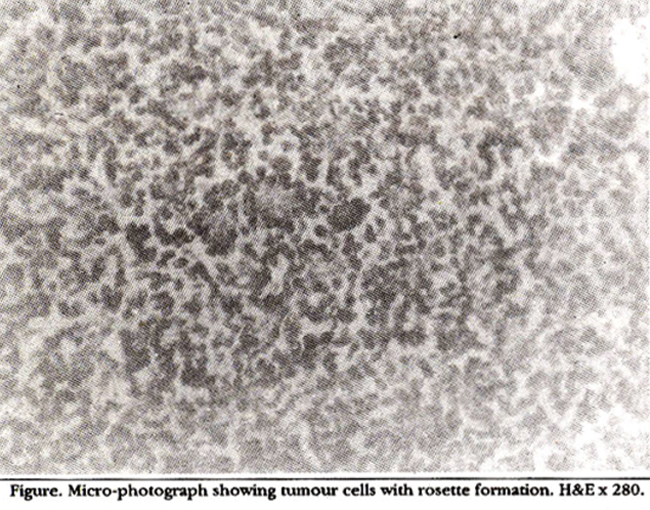
Histological examination of representative serial sections showed replacement of entire renal architecture by sheets of small, ill defined cells having hyperchromatic nuclei and a thin rim of cytoplasm. These cells were larger than lymphocytes. In most of the areas tumour cells were not forming any organoid pattern but in some areas characteristic Holmer Wright rosettes were present. A few areas of haemorrhages and necrosis were also seen. In addition a few trapped glomeruli and tubular structures were observed within the bands of fibrous tissue. These features were consistent with the diagnosis of a “neuroblastoma of the Kidney" The accompanied adrenal gland showed normal morphology.
DISCUSSION
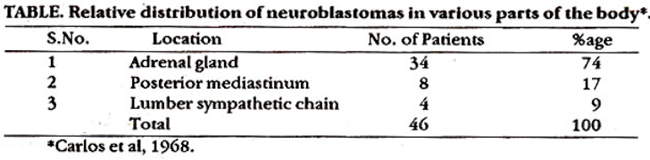
Neuroblastoma is one of the most common solid tumours of childhood. As they arise from the cells of neural crest, these may be found in a variety of situations5. Table shows the location of neuroblastomas in consecutive 46 cases reported by Carlos6. Apart from adrenal medulla, neuroblastomas have been reported in the brain, bone marrow, posterior mediastinum, pelvis and in relation to the olfactory nerves. Adrenal neuroblastomas locally invade the surrounding tissues and often extend into the kidney. Exceptionally the whole neoplasm is found within the kidney, the adrenal medulla being spared all together7. It has been postulated that these tumours arise from aberrant neuroectodermal cells which originate from the neural crest and amalgamate with the developing renal tissue8. The neural crest origin of this tumour has been confirmed by the detection of specific CNS proteins in tissue culture of the tumour cells9. Under rare circumstances these sequestrated cells undergo malignant change and give rise to a neuroblastoma10. Histologically the cells are small and dark like lymphocytes and are frequently arranged in masses without any specific pattern. In a characteristic lesion rosettes are formed where the tumour cells occupy the periphery and young nerve fibrils grow into the centre of each rosette. These features help to differentiate it from a nephroblastoma in which the characteristic features are primitive glomeruli with poorly formed Bowman’s spaces and abortive tubules enclosed within a spindle cell stroma11,12. Age affects the prognosis for the victims of this dreadful malignancy. The prognosis is bad between the ages of 2 and 6 years13 but it does not further worsen afterwords14. Although extra adrenal neuroblastomas have been shown to have better prognosis15, it is not certain that the similar tumours of the kidney are also associated with better survival rates.
REFERENCES
1. Reiselbacb. RE. and Garnick, M.B. ed. Cancer and the kidney. Philadelphia, Lea and Febiger, 1982, pp. 294-95.
2. Evans, A.E. Staging and treatment of neuroblastomas. Cancer, 1980;45:1799-802.
3. Kogut, M.D. and Donnell, G.N. Cushing’a syndrome in association with renal ganglioneuroblastoma. Paediatrics, 1961;28:566-77.
4. Mostofi, F.I., Sesterbenn, l.A. and Sobin, LH. Neuroblastoma; a primary tumourof the kidney in histological typing of the kidney tumours. International histological classification of tumours. Geneva, WHO., 1981, p.22.
5. Murphy, M.L. Curability of cancer in children. Cancer, 1968;22:779-84.
6. Carlos, A.P.,Teresa, J.V., Lauren, V.A., Kulapongs, P. and Powers, W.E. Treatmentof the malignant sympathetic tumours in children: clinicopathological correlation. Paediatric, 1968;41:45262.
7. Rosai, J.M. Neuroblastoma, in Ackerman’a surgical pathology. 6th ed. Saint Louis. Moaby, 1981, pp. 705-7.
8. D\\\'Angio. C.J.. Evans, A.E. and Koop, C.E.Special pattern ofwidespread neuroblastoma with a favourable prognosis. Lancet, 1971;1:1046-49.
9. Herschman, H.R. and Lerner, M.P. Production of a nervous system specific (14.3-2) protein by human neuroblastoma cells in culture. Nature, 1973;24:242-46.
10. Bennington, .J.L. and Beckwith, J.B. Secondary tumours involving the renal pelvis and ureter. Tumours of the kidney, renal pelvis and ureter. Washington, Armed Forces Institute of Pathology, 1983, pp. 319-24.
11. Waisnaan, 3. Theadrenal glands, in surgical pathology. Edited by F.W. Coulson. 2nd ed. Philadelphia, Lippincott, 1988, vol.2. pp. 948-49.
12. Cohen, H.A. The urinary tract, in surgical pathology. Edited by F.W. Coulson. 2nd ed. Philadelphia, Lipincott, 1988,vol. 1, pp.512-13.
13. Sutow, W.W., Gehan, LA., Heyn, R.M., Kung, F.H., Miller, LW., Morphy, ML. and Traggis, D.G. Comparison of survival curves, 1956 versus 1962, in children with Wilm\\\'s tumourand neuroblastoma. Paediatrics, 1970 45:800-11.
14. Wilson, L.M. and Draper, G.J. Neuroblastoma, its natural historyand prognosis; astudy of487caaes. Br.Med.J., 1974;3:301-30.
15. Haber, S.L. and Bennington, J.L. Maturation of congenital extraadrenal neuroblastoma. Arch. Pathot, 1963;76:121-28.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: