
Mirza Naqi Zafar ( Ziauddin Hospital Laboratory, Karachi. )
Serajuddaula Syed ( Ziauddin Hospital Laboratory, Karachi. )
April 1992, Volume 42, Issue 4
Original Article
ABSTRACT
Most laboratories in Pakistan use expensive imported clinical chemistfy feagent kits resulting in high cost/test to the patients. To reduce these costs, reagents were prepared from basic chemicals, substrates and enzymes imported from Sigma Chemical Company U.K. This reduced the cost/test by upto 500% in some reagents. The quality of these reagents was tested by Wellcome External, Q.C. Locally prepared reagents were comparable to or better than commercial reagents systems in terms of accuracy and precision. This paper describes the preparations according to I.F.C.C., costs and quality control of some of the reagents i.e., glucose, calcium, bilirubin, albumin, total protein, urea, ALT, AST and LDH and their comparisons with equivalent commercial kits (JPMA 42: 95, 1992).
INTRODUCTION
In Pakistan most laboratories use chemistry kits imported from Europe or U.S.A. These kits are costly due to weaker local currency, duties and taxes. Hence cost/testis high and this in turn becomes a burden on the patient The per capita income of Pakistan is Rs. 7,700 ($350) and the charges of routine tests like LFT Rs.200 ($10), glucose Rs. 50 ($2) and cardiac enzymes Rs. 300 ($14) are thus far too high for our poorer patients. To reduce the cost in-house preparation of clinical chemistry reagents systems from basic chemicals, substrates and enzymes imported from Sigma Chemical Company U.K. was started. In Pakistan there are no duties or taxes on self user import1. This paper describes the methodologies according to I.F.C.C., costs and quality assessments of some of our reagents systems. It also compares economy and quality of in-house reagents systems to that of commercial reagent systems.
MATERIALS AND METHODS
All basic chemicals substrates and enzymes for the preparation of the following reagent systems, glucose, urea, creatinine, protein, albumin, bilirubin, calcium, ALT, AST, alkaline phosphatase and LDH were imported from Sigma, U.K.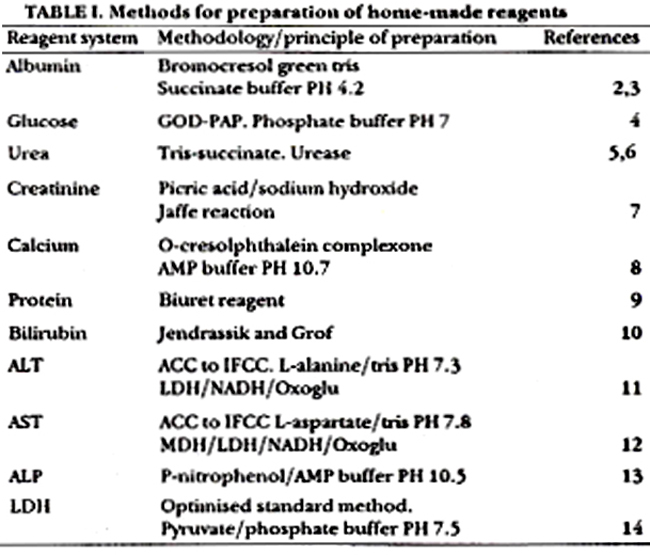
Table I lists the detailed methodologies used with appropriate preparation references2-12. The shelf life of these home-made and commercial reagents were tested and checked for periods of weeks, months an, in some, upto a year by analysing commercial quality control sera, precinormU and precipath U (Boehringer). The quality, accuracy and precision of home-made reagents were tested using commercial controls (Boehringer) as reported earlier13 and by Wellcome External Quality Control Scheme. These three modalities of QC were compared with those obtained with commercial reagent systems obtained from Boehringer and Merck. Wellcome QC results were followed for 6 months cycles each for the home-made and commercial reagent systems and data analysed from Wellcome results. In-house quality control data was established by running the two reagent systems for 3 months cycles. The cost/test of home-made and commercial kits was determined by considering firstly cost of commercial reagent kit divided by number of tests possible. The cost/test of home-made reagent was then calculated by estimating the total cost required to manufacture an equivalentvolume or reagent divided by the number of tests. All tests were performed on Hitachi 705 auto- analyser.
RESULTS
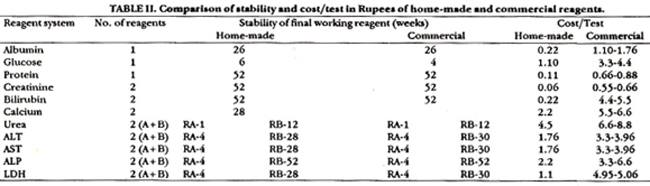
Table II lists the stabilities of the final reagent mixtures of home made and commercial reagents after placement in the autoanalyzer. In chemistries where two reagents are used, low stabilities were found due to unstable nicotinamide adenine dinucleotide compounds except for ALP where the substrate p. 2-4 dinitrophenol is unstable and dissociates with time. Home-made reagent stabilities are comparable to commercial reagent systems. Table II also shows cost/test in rupees of the home-made reagent systems compared to the commercial kits Boehringer, Merck and AMES. One US dollar is taken as equivalent to 22 Pakistani rupees. The home-made reagents are on the average 100 to 500% cheaper.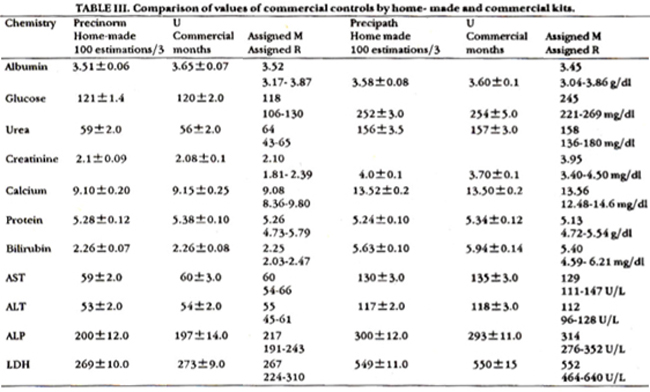
Table III shows values of commercial controls obtained by two reagent systems. Results are mean of 100 observations taken over a period of three months for the two systems. Both reagent systems give comparable results when compared to the manufacturers assigned mean (M) and range (R).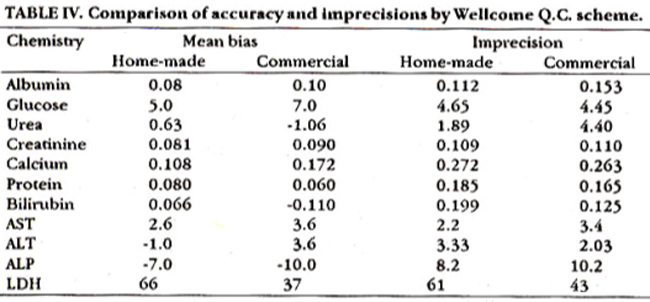
Table IV shows a comparison of accuracy and imprecision data by Wellcome QC for the two reagents systems. Each system was run for 6 monthly cycles. All chemistries are comparable except homemade reagents gave better performance for urea and poorer for LDH.
DISCUSSION
Advantages of home-made kits include reduced cost/test and long stability of reagents. Most require twice yearly manufacture, exceptions are systems where NADH is used. Its unstabiity requires weekly NADH preparations. This problem is overcome by using preweighed vials of the coenzyme making these systems similar to the commercial kits. The quality of home-made reagent systems are comparable to commercial kits and all these chemistries had high standings on the Welcome Q.R. league table. A routine problem most laboratories encounter is the nonavailability of commercial kits resulting in frequent change from one system to another specially when normal ranges differ. This problem is completely alleviated by home-made reagents. Our only shortfall is dependence for supply of standards or calibrators and control sera from commercial firms. We have already started preparation of in-house quality control sera and their efficacy and reliability is being tested. We continue to manufacture and use our reagent systems and strongly recommended high volume laboratories to initiate in- house manufacture. Perhaps then the suppliers of commercial kits will reduce their profit margins allowing ease to all laboratories both high and low volume.
REFERENCES
1. Import Trade Control Schedule, Government of Pakistan, Karachi, Manzoor Press,1981, Sec. 4, pp. 50-1.
2. Kachmar, J.F. and Grant, G.H. Proteins and amino acids in fundamentals of clinical chemistry. Edited by Norbert W. Tietz, Philadelphia, Saunders, 1987, pp. 337-8.
3. Doumaa, B.T. and Bigga, H.C3. Determination ofaerum albumin, in atandard methoda in clinical chemistry. Edited by G.A> Cooper. New York, Academic Preas, 1977, v. 7, pp. 175-6.
4. Variey, H., Gowenlock, A.H. and Bell, M. Blood glucoae and its determination, in practical clinical chemistry. 5th ed. London, William Heinemann, 1980, v. 1, pp.389-90.
5. Gutmann, I. and Bergmeyer, H.V. Methods of enzymatic analysia. Editor: H.U. Bergmeyer. 2nd English ed. New York, Academic Press, 1974, pp. 1791-3.
6. Boehringer Mannheim.Testcombination urea instruction manual. GmbH. Manriheim, 1989, pp. 122-3.
7. Larsen, K. Crestinine assay by a reaction kinetic principle. Clin. Chim. Acts, 1972; 41:209-13.
8. Moorehead, W.R. and Biggs, H.G. 2-Amino-2-Methyl-I-Propanol as the alkalyzing agent in an improved continuous [low cresolphathalein complexone procedure for calcium in serum. Clin. Chem., 1974; 20:1458-61.
9. Wootten, LD.P. and Freeman, H. Biuret method for total serum protein, in microanalysis in medical biochemistry. 6th ed. London, Churchill Uvingstone, 1982, pp. 144-5.
10. Routh, 3.1. Liver function, in fundamentals of clinical chemistry. Edited by Norbert W. Tietz. Philadelphia, Saunders, 1976, pp. 1026-62.
11. Kachmar, J.F. and Moss, D.W. Enzymes, in fundamentalsofclinical chemistry. Edited by Norbert W.TIetz. Philadelphia, Saunders, 1976, pp. 677-82.
12. Vsrley, H., Gowenlock, A.H. and Bell, M. Enzymes, in prscticalclinicalbiochemistry. 5th ed. London, William Heinemsnn, 1980, v.1, pp.717-8.
13. Lalani, It, Zafar, M.N. and Khurshid, M. Efficacy ofinternalsnd external qualitycontrol in chemical pathology. J. Pat Med. Assoc., 1988; 38:255-9.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: