
Muhammad Shafique ( Department of Biochemistry, Quaid-i-Azam Medical College, Bahawalpur. )
Misbah-ul-Ain ( Department of Biochemistry, Islamia University, Bahawalpur. )
Muhammad Ashraf ( Coronary Care Unit, Bahawalpur Victoria Hospital, Bahawalpur. )
April 1993, Volume 43, Issue 4
Original Article
ABSTRACT
Twenty-two patients receiving long term diuretic treatment for arterial hypertension (19) and congestive heart failure (3) received magnesium chloride 10 mmol/day for four months. Both systolic and diastolic pressures decreased significantly, by a mean of 13±9 mmHg. No significant changes were recorded in serum or urinary electrolytes except for magnesium (JPMA 43: 77, 1993).
INTRODUCTION
Disturbances of magnesium metabolism may have profound effect on the contractile state of vascular smooth muscle and thus on blood pressure1. Thiazides, prescribed to treat arterial hypertension, induce major changes in both the external and internal electrolyte balance and magnesium influences the relation between extra-cellular and intracellular potassium2. Effects of magnesium supplementation on electrolytes and blood pressure in patients receiving long term diuretic treatment for hypertension are reported here.
PATIENTS AND METHODS
Twenty-two (14 females, 8 males) patients between the ages of 38-70 years attending the cardiac units of B.V. Hospital, Bahawalpur were selected for this study. All were on diuretics for more than one year. The diuretics used were bendr of luazide (2.5mg/day) hydrochlorothiazide (12.5 mg/day) and frusemide (40 mg/day) along with potassium supplementation. All patients were administered 10 mmol magnesium chloride/day (243 mg magnesium or 2033 mg MgCl2, 6H2O/day) filled in empty capsules, corresponding to the recommended daily intake for up to four months. None of the patients was taking any other drug known to influence the metabolism of magnesium. On admission for study, the patients were seen twice at an interval of two to three days. Blood pressure and heart rates were recorded in supine position after 30 minutes rest and then in the standing position. Body weights were determined. Blood samples before and after magnesium supplementation were obtained for the analysis of electrolytes and creatinine and 24 hour urine was also collected for the estimation of electrolyte excretion. For comparison, a control group of 20 hypertensive patients (13 females and 7 males) of same age range, receiving almost similar diuretics, were selected from the same cardiac units. Student’s ‘t’ test was used for the assessment of statistical significance.
RESULTS
The comparative basic data of patients and controls is shown in Table I.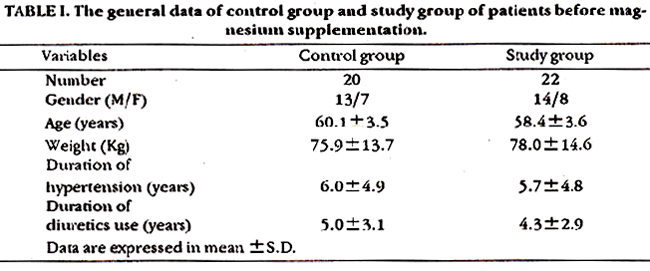
In the treatment group 21 of the 22 patients showed a decrease in blood pressure. In four patients the magnesium dosage had to be reduced to 406 mmol/day (97±146 mg magnesium or 813±1820 mg MgCl2 6 H2O/day) because of low blood pressure and dizziness. In five patients the thiazide dosage was reduced. Despite these therapeutic changes both supine and standing blood pressure had fallen significantly (P<0.001 and P <0.05 respectively) after four months treatment with magnesium (Table II).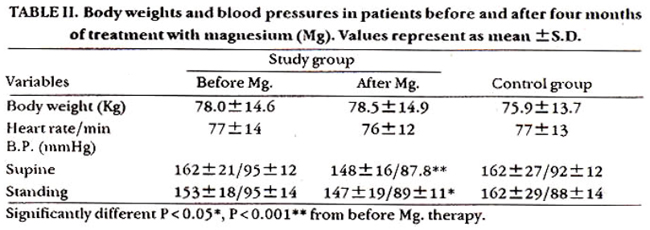
However, the difference in the heart rates before and after magnesium use was not significant. The alterations in blood pressure and heart rate in control group which was not receiving magnesium did not change significantly after four months. Magnesium therapy had no’ significant effect on serum electrolytes. There was a slight increase in urinary excretion of magnesium and sodium but no change in potassium excretion (Table III).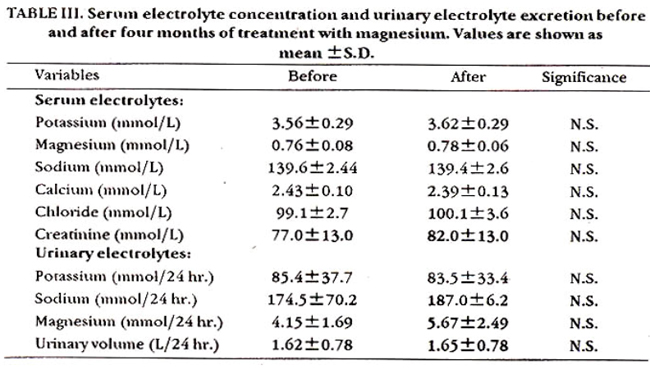
Magnesium had no effect on body weight and 24 hours urine volume (Table II and III).
DISCUSSION
Changes in electrolytes occur in patients on diuretic therapy. Prolonged use of thiazides results in deficiency of magnesium and potassium and an increase in the cellular sodium content. This may result in increased cellular calcium content and possibly vaso constriction3. This may be one of the factors necessitating additional treatment to control blood pressure in some patients after along term diuretic therapy. In this study of hypertensive patients already receiving diuretics a reduction of 13/9 mmHg was achieved with magnesium supplementation. This therapy should therefore be considered as an additional treatment in hypertensives receiving diuretics.
ACKNOWLEDGEMENT
This work was partially supported by the Bahawalpur Heart Society. Help of Prof. Iqbal Ahmad Khan, Principal Q.M.C. Bahawalpur and Dr. Ghulam Mustafa in the preparation of manuscript and management of patients, Mr. Sajjad Hussain for statistical analy sis and Mr. Shafi Mohammad for secretarial assistance is gratefully acknowledged.
REFERENCES
1. Altura, B.M. and Altura, B.T. Role of magnesium ions in contractility of blood vessels and skeletal muscles. Magn. Bull., 1981; 1a:102-14.
2. Dyckner, T. and Wester, P.O. The relation between extra and intracellular electrolytes in patients with hypokakmia and/or diuretic treatment. Acts. Med. Scand., 1978; 204:269-82.
3. Simpson, F.O. Salt and hypertension: a sceptical review of the evidence. Clin, Sci., 1979; 57 (Suppl. 5):463-80s.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: