
B. Ali ( Department of community Health Sciences, The Aga Khan University Hospital, Karachi. )
M. Saud ( Department of community Health Sciences, The Aga Khan University Hospital, Karachi. )
S.N. Mohammad ( Department of community Health Sciences, The Aga Khan University Hospital, Karachi. )
M. Lobo ( Department of community Health Sciences, The Aga Khan University Hospital, Karachi. )
F. Midhet ( Department of community Health Sciences, The Aga Khan University Hospital, Karachi. )
S.A. Ali ( Department of community Health Sciences, The Aga Khan University Hospital, Karachi. )
April 1993, Volume 43, Issue 4
Original Article
ABSTRACT
A cross-sectional observational systematic study was carried out on ambulatory patients at a tertiary care hospital to determine the probable prevalence, associated factors and significance of psychiatric morbidity by using an Urdu translation of the hospital anxiety and depression (HAD) scale over a period of 6 days in a week. Results showed a prevalence of 38.4% which is slightly higher than what has been generally reported (30%). Two variables, i.e., female sex and being a housewife were significantly related with the outcome. An attempt has been made to identify the probable reasons for this and some suggestions laid down for further work (JPMA43: 69, 1993).
INTRODUCTION
“Mental disorder is part of life itself”, Arthur Kleinman. A study was conducted to estimate the prevalence of psychiatric morbidity and its associated risk factors in ambulatory patients of Aga Khan University Hospital. Goldberg1 has reported a prevalence of psychiatric illness of 30% in general medical patients. Goldberg and Huxley2 further said that out of 250 psychiatric patients per 1000 per year, 230 were accessible to primary care. Meagre data exists on psychiatric, morbidity in Pakistan with Mumford and Tareen3 reporting an average prevalence of 30% in general hospital settings. Goldberg and Bridges4 have stated that anxiety and depression are the commonest psychiatric problems seen by general physicians when they found that of 590. patients presenting to their general practitioners with a new complaint, 31.6% were diagnosed to have anxiety or depression. Other DSM III diagnoses accounted for only 1.5% of cases. Accordingly it was decided to use anxiety and depression as indicators of psychiatric morbidity.
SUBJECTS AND METHODS
A descriptive cross sectional study was carried out at Community Health Centre a general walk in cum appointment clinic, at AKUH. Eligibility for inclusion in the study were patients 16 years and older. Over a period of one week a total of 180 patients were selected by systematic random sampling, of which 167 completed the interview. The reasons for dropping out were need for urgent medical care, language problem and refusal to participate after seeing the forms. The hospital anxiety and depression (HAD) scale5 was chosen as the instrument for data collection as it has been designed for use in outpatient departments of non-psychiatric hospitals. A validated Urdu translation of the I-LAD scale3 was used in this study and a score of 11 or above was kept as the cut off point. Informed consent was obtained and data was collected using the HAD scale. In addition, Socio demographic information (age, sex, marital status, occupation, family income) and family history of psychiatric illness was also recorded.
RESULTS
Analysis of data revealed that of the 167 people interviewed, 64 were screened positively for psychiatric morbidity, giving a point prevalence of 38.4%. The distribution being anxiety - 19.2%, depression - 4.2% and anxiety with depression - 15%. Psychiatric morbidity was found to be significantly associated with females and housewives. Only five people who were screened positive on HAD scale for depression had a positive family history of psychiatric morbidity. No significant association (P=O.05) was found between income arid psychiatric morbidity but the data suggests that an association may exist (Table).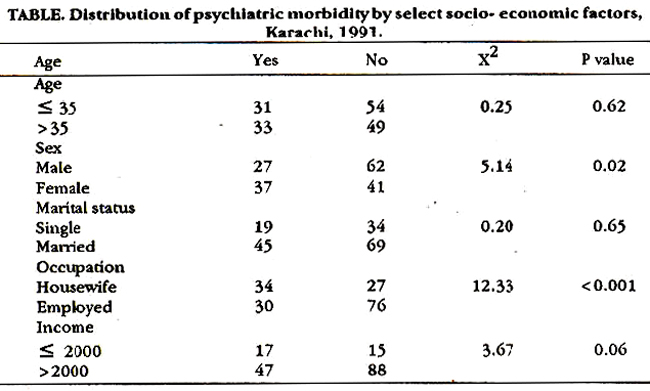
DISCUSSION
A prevalence of 38.4% in a general clinic of tertiary care hospital (AKU) could probably be explained by the fact that anxiety and depression are masked by somatic symptoms often leading to unnecessary delays in diagnosis and management6 thus compelling patients to seek relief at tertiary care facilities. A high level of civilian stress7 that exists in Karachi could also explain the high prevalence found in this study. A large community based study is being planned to determine whether the reported prevalence is also true in a community Setting. Our study demonstrates that the female sex had higher psychiatric morbidity which is in consonance with medical literatures8. Studies in the West have shown that lack of paid employment increases the vulnerability of women to depression9. The relationship between household income and psychiatric illness has been documented7 and results from our study show that there is a strong possibility of this in the population studied. Only 5 of the cases admitted to a family history of psychiatric illness which can probably be explained by the taboos and stigmas associated with the problem. A prevalence of 38. 4% in a general clinic, calls for a review of medical, nursing and public health education and practice in Pakistan, possibly on the lines of the USA medical school curriculum10. In addition, mental health care needs to have an allocation in the National Health Policy which is proportionate to the prevalence of psychiatric problems6. Further attempts need to be made at developing highly focussed socio therapeutic and preventive interventions at the community level11.
ACKNOWLEDGEMENT
We would like to acknowledge the help and support of Farzana Diwani, Akber Hashim and Saquib Nadeem without whose help we would not have been able to conduct this study.
REFERENCES
1. Goldberg, D.P. identifying psychiatricillnessamonggeneral medical patients. Br.MedJ., 1985;291:161-2.
2. Prestige, B.R. and Lake, CR. Prevalence and recognition ofdepreasion amongprimasy care outpatients. J.Fam.Pract., 1987;25:67-72.
3. Mumford, D.B., Tareen, I.A.K., Bajwa, M.A.Z., Bhatti, M.R. and Karim, It The translation and evaluation of Urduversion of the hospital anxiety and depression scale. Acta Psychiatr. Scand., 1991;83:81-5.
4. Goldberg, D. and Bridges, K. Screening for psychiatric illness in general practice: the general prsctitionersversus the screening questionnaire. J.R.Coll.Pract., 1987;37:15-8.
5. Zigmand, AS. and Snaith, R.P. The hospital anxiety and depreaaion scale. Acts Psychiatr. Scand., 1983;67:361-70.
6. Ndetei, D.M. and Muhangi, 3. The prevalence and clinical presentation of psychiatric illness ins rural setting in Kenya. Br.). Psychiatry, 1979;135:269-72.
7. Weismsn, M.M. and Kleinman, G.L. Epidemiology of mental disorders. Arch. Gen. Psychiatry, 1978;35:705-12.
8. Psykel, ES. Depression in women. Br3.Psychiatty, 1991;1S8 (Suppi 10):22-9.
9. Britchnell, 3., Masters, N. and Deahl, M. Astudy ofyoungmarried women on a London housing estate. Br.J. Psychiatry, 1988;153:56-64.
10. Kaplan, HI. and Ssdock, B.). Behavioural sciences and clinical psychiatry. Synopsis of psychiatry. Baltimore, Willisms and Wilkins, 1988, preface p.5.
11. Kleinmsn, A Rethinking psychiatry. From cultural category to personal experience. New York,The Free Press, 1991, p. 174.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: