
Saadia Ilyas ( Muhammadi Hospital, International Medical Research Centre, Pakistan Heart Foundation, Hayatabad, Peshawar. )
Hajira Ilyas ( Queen’s Hospital, Romford, Essex, UK. )
Abdul Hameed ( Children B-Ward, Khyber Teaching Hospital, Peshawar. )
Muhammad Ilyas4 ( Muhammadi Hospital, International Medical Research Centre, Pakistan Heart Foundation, Hayatabad, Peshawar. )
September 2013, Volume 63, Issue 9
Case Reports
Abstract
A case report of 6-year-old boy with progeria syndrome, with marked cardiac complications is presented. The boy had cardiorespiratory failure. Discoloured purpuric skin patches, alopecia, prominent forehead, protuberant eyes, flattened nasal cartilage, malformed mandible, hypodentition, and deformed rigid fingers and toes were observed on examination. The boy was unable to speak. A sclerotic systolic murmur was audible over the mitral and aortic areas. Chest x-rays showed cardiac enlargement and the electrocardiogram (ECG) showed giant peaked P waves (right atrial hypertrophy) and right ventricular hypertrophy. Atherosclerotic dilated ascending aorta, thickened sclerotic aortic, mitral, and tricuspid valves with increased echo texture, left and right atrial and right ventricular dilatation, reduced left ventricular cavity, and thickened speckled atrial and ventricular septa were observed on echocardiography.
Keywords: Progeria syndrome, Cardiorespiratory failure.
Introduction
In 1886, Jonathan Hutchinson succinctly reported a 4-year-old boy looking like an old man.1 Almost two decades later, a second similar case was reported, which was thereafter named Hutchinson-Gilford progeria syndrome (HGPS).2 Accelerated or premature aging (progeria) is a very rare genetic disorder, occurring in 1 per 4,000,000 live births; males are affected 1.5 times more than the females, and most cases have been reported from the Caucasians. Progerin accumulation is considered to be the cause of the disorder. Survival is restricted to the teenage, and death occurs mostly due to respiratory infections, congestive cardiac failure, myocardial infarction and stroke.
A child with progeria is borne normally; dysmorphic features appear with age. These include retarded growth, narrow chest, baldness, macrocephaly, pinched beaked nose (bird-like face), and protuberant eyes with the absence of eyebrows and lashes. The skin appears senile with spots along with loss of subcutaneous fat. A deformed oral cavity is found with irregular teeth. Fingers and toes are malformed; musculoskeletal abnormalities occur due to osteoporosis and skeletal dysplasia, with swollen stiff joints and hip dislocations. Presence of abnormal collagen, causing generalised atherosclerosis, leads to most deaths, which are due to fatal cardiovascular or cerebrovascular vasculopathy in children and adolescents. The causative progerin is a possible clue to the control of senilism. The synonym senilis cordis is generally implied for atherosclerotic cardiovascular pathology (cardiac sclerosis) due to the aging process over the age of 60 years.
Case Report
A 6-year-old boy (M.M.) from Peshawar was referred from the Children-B Ward of Khyber Teaching Hospital, Peshawar with presenting complaints related to chest infection for the preceding 6 weeks and symptoms of cardiac failure for 18 months. The features of abnormal growth and aging were noticed at 2.8 years (Figure-1).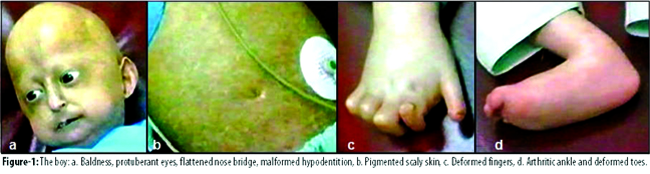
He had a normal elder 9-year-old brother.
On examination, reduced height and body mass index (BMI), alopecia, prominent forehead, protuberant eyes, flattened nose bridge, deformed hypodentition, deformed mandible, and dry sclerodermic purpuric skin patches over the abdomen and limbs were observed. The hands and feet were small with malformed rigid fingers and toes. Hearing was within normal limits, but the boy was unable to speak. Pulse was 144 beats per minute and the blood pressure was 90/70 mmHg. Crepitations in the lung fields and a proto-diastolic gallop were audible. A short systolic (sclerotic) murmur was audible over the mitral and the aortic areas and signs of congestive cardiac failure were present. On laboratory investigations, haemoglobin was found to be 9.3 G/dl, urea was 47mg/dl, and serum cholesterol was 187mg/dl. Chest x-rays showed cardiac enlargement, and the electrocardiogram (ECG) showed right atrial hypertrophy with giant peaked P waves (leads II, III and aVF) and right ventricular hypertrophy (Figure-2).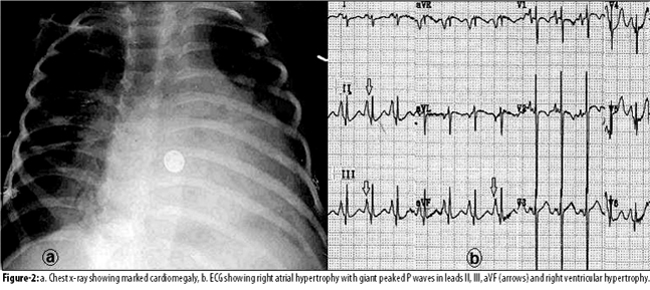
On 2D echocardiography, atherosclerotic dilated ascending aorta with sclerotic aortic valve (Vmax 188/second), thickened sclerotic mitral valve (MVA 1.3 cm2), and aortic and tricuspid valves with increased echo texture were recorded. Right and left atrial and ventricular dilatations and thickened speckled atrial and ventricular septa were recorded. M-mode showed thickened sclerotic mitral leaflets (Figure-3).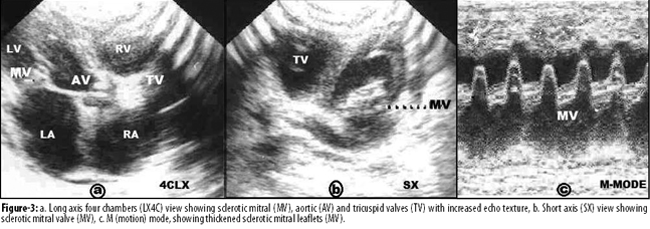
Discussion
Since the earlier reports of the first two recorded cases,1,2 reports on progeria have been few and far between. A survey by the Progeria Research Foundation confirmed that only 80 known children with progeria, 5 months to 21 years of age, were living across the world in August 2011.3 The first case of progeria in Pakistan was reported in 2008.4
Progeria, or accelerated aging ("geras" for old age in Greek), is a very rare genetic disorder, with an incidence of 1 in 4,000,000 live births. It is caused by mutation of lamin-A gene, which replaces cytosine by thymine to form an unusual form of lamin-A protein (progerin) that normally forms the nuclear envelope. Vascular progerin generation significantly increases throughout life with effect on cardiovascular aging. Abnormal collagen leads to generalised atherosclerosis, which causes death due to myocardial infarction and stroke. Abnormal accumulation of progerin is considered to be the cause of progeria, and most of the cases die at early ages of 7-20 years due to heart failure, myocardial infarction and stroke.
The first case from Pakistan of a 6-year-old girl with progeria4 reported retarded growth, alopecia, senile skin, macrocephaly, protruding eyes with loss of eyebrows and eye-lashes and thin beaked nose, micrognathia, malformed oral cavity with discoloured crowded irregular teeth. She had anaemia, elevated serum lipid levels, and increased hyaluronic acid level in the urine. On radiological investigation, calcification in soft tissues around multiple joints, skull diastasis of the sagittal suture, hypoplastic mandible, osteoporotic ribs and clavicles, and terminal resorption of phalanges were seen. The ultrasonographic and electrocardiographic findings were normal.
We are reporting herein a 6-year-old boy with progeria, who presented with respiratory infection and cardiac failure and was confirmed to have cardiovascular atherosclerotic changes, which included a characteristic systolic (sclerotic) murmur of valvular sclerosis, and signs of congestive cardiac failure. Chest X-rays showed cardiomegaly and the electrocardiogram showed right atrial and ventricular hypertrophy. Echocardiography confirmed dilated atherosclerotic aortic root with septal involvement, and thickened sclerotic aortic, mitral and tricuspid valves, with atrial dilatation and systolic and diastolic ventricular dysfunctions.
In 31 typical reported cases of progeria, cardiac murmurs were common after the age of 5 years, with systemic (diastolic) hypertension, cardiomegaly, and hypercholesterolaemia developed in many cases.5 In 15 children (1-17 years) with progeria, prolonged prothrombin time, raised serum phosphorus level, insulin unresponsiveness, and growth hormone deficiency, elevated blood pressure and decreased ankle-brachial indexes, were common. Growth hormone treatment in a few patients increased growth by 10% and weight by 50%.6 In progeria, the carotid-femoral pulse wave velocity was significantly elevated with echo brightness of the carotid arterial texture.7
Coronary atherosclerosis and prominent adventitial fibrosis with high level of progerin were demonstrated on autopsy of 2 children with progeria who died due to myocardial infarction.8 Two unrelated young women with LMNA gene mutation, and similar features of accelerated aging, presented with progressive dilated cardiomyopathy and had premature ovarian failure.9 LMNA, a complex protein of the mammalian nuclear lamina, is encoded with the LMNA gene. A mutation of prelamin causes progeria. Children with progeria are advised a high-calorie diet, protection against infection, small daily dose of aspirin and lipid-lowering drug (statin) to prevent heart attack and stroke. Physiotherapy is required for prevention of injuries. A bisphosphonate drug to protect bones may be used. A farnesyltransferase inhibitors (a progerin-blocker drug Rapamycin) has been experimentally reported to remove progerin in children with progeria.10
Conclusion
Progeria is a very rare disorder and is due to abnormal accumulation of progerin. The survival of progerian children is restricted to childhood and adolescents. Currently there are about 100 known living cases in the world. Studies on progerin may lend some clue to controlling premature senescence!
Acknowledgements
We are grateful to the medical and nursing staff of the Children-B Ward Khyber Teaching Hospital, Peshawar, and the Muhammadi Hospital-IMRC, Hayatabad, for all their assistance.
References
1. Hutchinson J. Congenital absence of hair and mammary glands with atrophic condition of the skin and its appendages in a boy whose mother had been almost totally bald from alopecia areata from the age of six. Med Chir Trans 1886; 69: 473-7.
2. Gilford H. Progeria: a form of senilism. Practitioner 1904; 73: 188-217.
3. Progeria Research Foundation. (Online) (Cited 2012 August). Available from URL: www.progeriaresearch.org/number-of-children-to-continue-to-soar.html.
4. Iqbal M, Iftikhar A. Progeria - first case report from Pakistan. Rawal Med J 2008; 33: 266-7.
5. Makous N, Friedman S, Yakovac W, Maris EP. Cardiovascular manifestations in progeria. Report of clinical and pathologic findings in a patient with severe arteriosclerotic heart disease and aortic stenosis. Am Heart J 1962; 64: 334-46.
6. Merideth MA, Gordon LB, Clauss S, Sachdev V, Smith AC, Perry MB et al. Phenotype and course of Hutchinson-Gilford progeria syndrome. N Engl J Med 2008; 358: 592-604.
7. Gerhard-Herman M, Smoot LB, Wake N, Kieran MW, Kleinman ME, Miller DT et al. Mechanisms of premature vascular aging in children with Hutchinson-Gilford progeria syndrome. Hypertension 2012; 59: 92-7.
8. Olive M, Harten I, Mitchell R, Beers JK, Djabali K, Cao K et al. Cardiovascular pathology in Hutchinson-Gilford progeria: correlation with the vascular pathology of aging. Arterioscler Thromb Vasc Biol 2010; 30: 2301-9.
9. McPherson E, Turner L, Zador I, Reynolds K, Macgregor D, Giampietro PF. Ovarian failure and dilated cardiomyopathy due to a novel lamin mutation. Am J Med Genet A 2009; 149A: 567-72.
10. Graziotto JJ, Cao K, Collins FS, Krainc D. Rapamycin activates autophagy in Hutchinson-Gilford progeria syndrome: Implications for normal aging and age-dependent neurodegenerative disorders. Autophagy 2012; 8: 147-51.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: