
Zahida Parveen Brohi ( Department of Obstetrics & Gynaecology, Isra University Hospital, Hyderabad Sindh, Pakistan. )
Aneela Sadaf ( Department of Obstetrics & Gynaecology, Isra University Hospital, Hyderabad Sindh, Pakistan. )
Uzma Perveen3 ( Department of Obstetrics & Gynaecology Unit-11, LUMHS Hyderabad Sindh, Pakistan. )
September 2013, Volume 63, Issue 9
Original Article
Abstract
Objective: To determine the etiology, clinical features and outcome of fulminant hepatic failure in pregnancy.
Methods: An observational hospital based study was conducted at Isra University hospital Hyderabad from 1st March 2009 to 28th February 2010. Total 1192 obstetric patients were admitted in obstetrics & gynaecology department during this period, of whom 52 were with Fulminant hepatic failure in pregnancy and were included in this study. A pre-designed structured proforma was used. All patients had clinical history and underwent a physical examination. Routine laboratory tests, liver function tests and viral serology were performed in all cases. All results were analyzed on statistical software SPSS version 11. Frequencies and percentages were calculated, the final outcome was recorded.
Results: Out of 52, 6(11.5%) presented in the first trimester, 4 (7.6%) in the second trimester and 42 (80.7%) were in their 3rd trimester of pregnancy. Etiology of the disease was Hepatitis E in 28(53.8%), Hepatitis B in 9 (17.3%), Hepatitis C in 7 (13.5%) HELLP syndrome in 7 (13.5%) and acute fatty liver of pregnancy in 1 (3.57%) case. Maternal mortality was 15(28.8%) and foetal mortality was 40 (77%). Only 12 (23.1%) new born remained alive.
Conclusion: Fulminant hepatic failure in pregnancy has very high foetal and maternal mortality which is mostly due to viral hepatitis E.
Keywords: Pregnancy, Fulminant hepatic failure, Hellp syndrome. (JPMA 63: 1168; 2013).
Introduction
Fulminant hepatic failure is defined as presence of encephalopathy within 8 weeks of development of clinical illness in the absence of clinical evidence of chronic liver disease.1 Fulminant hepatic failure is a rare and frightening event- frightening because of its abrupt onset, and possibly fatal outcome in many cases. Severe liver dysfunction in late pregnancy is a dramatic event because it can progress very rapidly to fulminating disease and also because two lives, that of mother and foetus are involved.2 The important causes of such an event are acute viral hepatitis ,acute fatty liver of pregnancy, preeclampsia associated liver disease and intrahepatic cholestasis of pregnancy.3 Pakistan is endemic for all types of hepatitis and hepatitis E is a disease of developing countries with improper sewage disposal and unclean water supplies,4 and it occurs here in both sporadic and endemic forms, documented epidemics have occurred in Sargodha, Abbotabad and Islamabad.5-7 The course of acute viral hepatitis is unaffected by pregnancy except in patients with hepatitis E (HEV) which is endemic in our region and can cause very high maternal and foetal mortality.8 The reason for this increased maternal morbidity and mortality during pregnancy are not clear, however It is possible that malnutrition and pregnancy appears to be a potential risk factor for viral replication and low immune status in Indian/Asian pregnant women.9 High foetal mortality could be due to in-utero foetal transmission of hepatitis results in foetal hepatitis.10 It is important to differentiate between severe acute viral hepatitis and pregnancy associated liver diseases like acute fatty liver of pregnancy. The epidemiology of both diseases needs to be defined in pregnant women in our region. Treatment options may be different, as prompt termination of pregnancy is usually required for improving the prognosis in acute fatty liver and HELLP syndrome.11 Long term prognosis may be different in both groups because recent studies suggesting that acute fatty liver can recur in subsequent pregnancies.12 These patients were referred from basic health units and secondary care hospitals in very late stages, In spite of freely available screening and diagnostic tests for viral hepatitis every patient can not afford it due to their high cost, so there is reluctance for tests in peripheral areas further delay in diagnosis as well as referral to tertiary care units and results in increased morbidity as well as mortality. The aim of this study was to determine the etiology and outcome of Fulminant hepatic failure in pregnancy in our population.
Patients and Methods
An observational and prospective hospital based study was conducted at Isra University hospital Hyderabad for one year from 1st March 2009 to 28th February 2010. The study was approved by the Institutional Ethics Committee of Isra University. Total 1192 obstetric patients were admitted in obstetrics and gynecology department during this period of whom 52 were with acute liver failure in pregnancy and they were included in this study. Patients with chronic liver disease or with fulminant hepatic failure but not completely diagnosed and discharged on request due to non affordability were excluded from this study. Once enrolled in the study, a pre designed structured proforma was used, the demographic information including name, age, address, socioeconomic status were recorded and patients were further asked for complete history including the obstetrical history and previous antenatal record if present was taken. A detailed clinical examination was performed in all patients and routine laboratory tests, liver function tests and viral serology were performed in all cases. Obstetrical examination with any obstetrical intervention as and when needed was done in a few patients. All patients with fulminant hepatic failure were managed with supportive care in the intensive care unit in collaboration with the department of gastroenterology and Hepatology.
Descriptive statistics were used in this study and percentages were calculated for qualitative variables like cause of fulminant hepatic failure, complications, maternal and foetal outcome. Mean±Standard deviation were calculated for age, duration of jaundice at admission, and laboratory investigations. SPSS version11 was used for all statistical analysis.
Definitions
Socioeconomic status: It was defined on the basis of monthly income, low socioeconomic group (monthly income
Maternal education: Maternal educational was divided into six categories depending on the level of education (Illiterate, Primary, Middle, High, Undergraduate and postgraduate.
Residence: These are arbitrary definitions.
* Urban: An Urban area was a central city and surrounding areas whose population was greater than 50,000.
* Rural: The rural area was defined as whose population was less than 2,500 residents.
Results
A total 52 patients with fulminant hepatic failure in pregnancy were admitted at Isra University Hospital between 1st March 2009 to 28th February 2010. The mean age of the patients was 29.04±8.40 years (range 17 years to 42 years). Majority of the patients 49 (94.2%) had not received antenatal care (Table-1).
The most common cause of hepatic failure was acute hepatitis E infection comprising 28 (53.8%), of whom 7 (13.4%) patients died. Total 37 (71.2%) patients delivered while 15 (28.8%) did not deliver. Six (16.2%) delivered patients had uterine packing due severe postpartum haemorrhage, evacuation of products of conception was required in 4(10.8%) patients. The most common complication was encephalopathy found in 16 (30.8%) patients (Table-2).
Overall maternal mortality was 15 (28.8%), of which 3 (20%) were due to pregnancy associated liver failure, while 12 (80%) were due to viral hepatitis. Of the 37(71.2%) surviving patients, 24(64.8%) had complete recovery of liver function; 13(35.1%) had partial recovery. Foetal and perinatal outcome of delivered patients showed miscarriage in 4 (7.7%), preterm delivery in 2 (3.8%), stillbirth 15(28.8%), neonatal death in 4 (7.7%) and 12 (23.1%) new born remained alive (Table -3).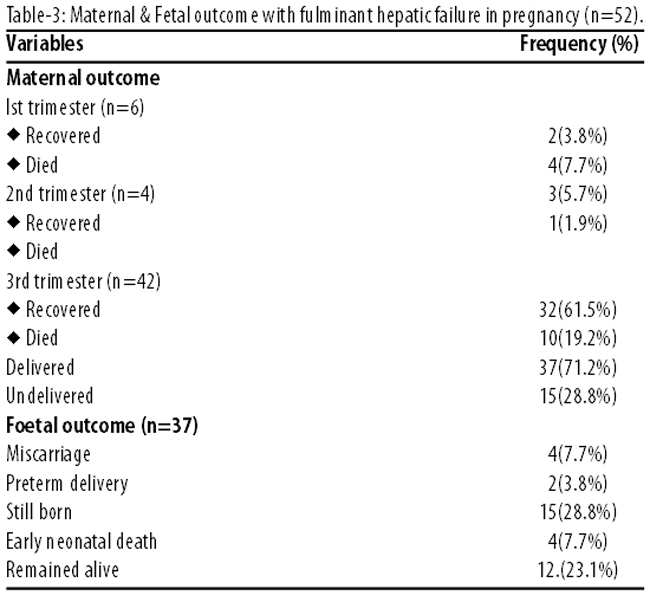
Discussion
In the present study, maternal mortality was seen in 29% and neonatal in 77% cases indicating viral hepatitis and fulminant hepatic failure as an important cause of death in Pakistan. HEV infection (53.8%) was the most common cause for liver failure with a mortality of 13.4%. Saeed et al reported much better prognosis in HEV patients than in other groups with severe liver failure.13 The attack rates in pregnant females have been reported from 17 to 40%.14 Aggarwal R reported HEV infection in 50-70% of all patients with sporadic viral hepatitis in India.15 while in another study the prevalence of HEV infection in third trimester was between 40-57%.16
Women with FHF secondary to hepatitis E appear to be more sick and have a higher mortality rate, possibly due to decreased metabolism leading to higher hormone levels and immune suppression.5 Estrogen is known to cause a reduction in thymus weight and can deplete the CD4 and CD8 cells and the development of T cells is blocked by progesterone.17 Some of the susceptibility during pregnancy may be due to a direct effect of high hormone levels on hepatic cells which may predispose to hepatic dysfunction with toxin or pathogen exposure as is seen with increased toxicity of the anti HIV multi drug regimen used together in pregnancy.18 The frequency of HBV associated FHF in our study was 17.3% while Jaiswal et al observed HBV infection in 19% cases.10 In this study Hepatitis C associated FHF accounts for 13.5%, while another study from our unit reported a lower frequency of 8% and no adverse effect on pregnancy outcome when compared to controls.19 Beniwal M et al have reported the same findings and did not find HCV associated FHF.20 The current study indicates very low frequency of acute fatty liver of pregnancy (1.9%), and same was fond by other workers.21 In our study the major complications of FHF were encephalopathy (30.8%) while Khuroo M.S found cerebral oedema (53.2%). Disseminated intravascular coagulation was similar in two studies.22 The foetal out come in our study was 4 (7.7%) miscarriages, 2 (3.8%) preterm deliveries, 15 (28.8%) still born, 4 (7.7%) early neonatal deaths and 12 (23.1%) babies remained alive. In comparison Mirghani found 2 (4.2%) miscarriages, 10 (20.8%) preterm, 2 (4.2%) stillborn and 36 (75%) term deliveries.23 High requency of abortions, stillbirths and neonatal deaths in pregnant women with hepatitis were reported by others too.24 In this study 66% deaths occurred in third trimester whichis lower than 80% reported by Mirghani, most of which occurred in post partum period.23 Various other studies on viral hepatitis showed 20% mortality rate in pregnant females in the second and third trimester.25
The present study has certain limitations that need to be taken into account: first are the small number of patients and second is that some patients were discharged on request and some could not afford the diagnostic tests, so their cause of liver failure could not be determined and they could not be included in the study.
Conclusion
Fulminant hepatic failure in pregnancy is a challenging clinical problem with very high maternal and fetal morbidity and mortality, viral hepatitis especially E was the most common cause of acute liver failure in pregnancy.
Early intervention and appropriate diagnosis can substantially reduce the morbidity and mortality associated with Fulminant hepatic failure especially in pregnancy associated acute liver diseases.
Proper disposable of waste, avoidance of contamination of food and the provision of pure water is recommended to prevent the outbreaks of hepatitis E (HEV) infection.
References
1. Khuroo MS, Rustgi VK, Dawson GJ, Mushahwar IK, Yattoo GN, Kamili S, et al . Spectrum of hepatitis E virus infection in India. J Med Virol 1994; 43: 281-6.
2. Riely CA. Acute hepatic failure in late pregnancy. (Online) 2010 (Cited 2010 December 22). Available from URL: www1.easl.ch/PGC/C.%20Riely.pdf.
3. Van Dyke RW. The liver in pregnancy. In: Zakim D, Boyer TD (eds). Hepatology: A Textbook of Liver Disease. Philadelphia: WB Saunders; 1990: 1438-59.
4. Shahzad F, Atiq M, Ejaz S, Hameed.S . Hepatitis E: review of a disease endemic in Pakistan. J Pak Med Assoc 2001; 51: 166-9.
5. lqbal M, Ahmed A, Qamar A, Dixon K, Duncan JF, Islam NU, et al. An outbreak of entericallv transmitted non-A, non-B hepatitis in Pakistan. Am J Trop Med Hyg 1989; 40: 438-43.
6. van Cuyck-Gandré H, Zhang HY, Tsarev SA, Warren RL, Caudill JD, Snellings NJ, et al. Short report: phylogenetically distinct hepatitis E viruses in Pakistan. Am J Trop Med Hyg 2000; 62: 187-9.
7. Rab MA, Bile MK, Mubarik MM, Asghar H, Sami Z, Siddiqi S, et aI. Water-borne hepatitis virus epidemic in Islamabad, Pakistan: a common source outbreak traced to the malfunction of a modern water treatment plant. Am J Trop Med Hyg 1997; 57: 151-7.
8. Malkani PK, Grewal AK. Observations on infectious hepatitis in pregnancy. Indian J Med Res 1957; 45 (Suppl): 77-84.
9. Jilani N, Das BC, Husain SA, Baweja UK, Chattopadhya D, Gupta RK, et al. Hepatitis E virus infection and fulminant hepatic failure during pregnancy. J Gastroentrol Hepatol 2007; 22: 676-82.
10. Singh S, Mohanty A, Joshi YK, Deka D, Mohanty S, Panda SK. Mother-to-child transmission of hepatitis E virus infection. Indian J Pediatr 2003; 70: 37-9.
11. Burroughs AK, Seong NH, Dojcinov DM, Scheuer PJ, Sherlock SV. Idiopathic acute fatty liver of pregnancy in 12 patients. Q J Med 1982; 51: 481-97.
12. Reyes H, Sandoval L, Wainstein A , Ribalta J, Donoso S, Smok G, et al. Acute fatty liver of pregnancy : a clinical study of 12 episodes in 11 patients. Gut 1994; 35:101-6.
13. Hamid SS, Jafri SM, Khan H, Shah H, Abbas Z, Fields H. Fulminant hepatic failure in pregnant women: acute fatty liver or acute viral hepatitis? J Hepatol 1996; 25: 20-7.
14. Lettau LA. The A, B, C, D and E of viral hepatitis: spelling out the risk for healthcare workers. Infect Control Hosp Epidemiol 1992; 13: 77-81.
15. Aggarwal R, Krawczynski K. Hepatitis E: An overview and recent advances in clinical and laboratory research. J Gastroentrol Hepatol 2000; 15: 9-20.
16. Jaiswal SP, Jain AK, Naik G, Soni N, Chitnis DS. Viral hepatitis during pregnancy. Int J Gynecol Obstet 2001; 72: 103-8.
17. Tibbetts TA, deMayo F, Rich S, Conneely OM, O\'Malley BW. Progesterone receptors in the thymus are required for thymic involution during pregnancy and for normal fertility. Proc Natl Acad Sci U S A. 1999; 96: 12021-6.
18. McGovern BH, Ditelberg JS, Taylor LE, Gandhi RT, Christopoulos KA, Chapman S, et al. Hepatic steatosis is associated with fibrosis, nucleoside analogue use, and hepatitis C virus genotype 3 infection in HIV-seropositive patients. Clin Infect Dis 2006; 43: 365-72.
19. Haider G, Zehra N, Munir A. Hepatitis C: frequency, risk factors, and pregnancy outcome. JSP 2009; 14: 33-7.
20. Beniwal M, Kumar A, Kar P, Jilani N, Sharma JB. Prevalence and severity of acute viral hepatitis and fulminant hepatitis during pregnancy: a prospective study from north India. Indian J Med Microbiol 2003; 21: 184-5.
21. Pockros PJ, Peters RL, Reynolds TB. Idiopathic fatty liver of pregnancy: findings in 10 cases. Medicine (Baltimore) 1984; 63: 1-11.
22. Khuroo MS, Kamili S. Aetiology, clinical course and outcome of sporadic acute viral hepatitis in pregnancy. J Viral Hepat 2003; 10: 61-9.
23. Mirghani OA, Saeed OK, Basama FM. Viral hepatitis in pregnancy. East Afr Med J 1992; 69: 445-9.
24. Tsega E, Hansson BG, Krawczynski K, Nordenfelt E. Acute sporadic viral hepatitis in Ethiopia: causes, risk factors, and effects on pregnancy. Clin Infect Dis 1992; 14: 961-5.
25. Usmanov RK, Balaian MS, Kazachkov IuA, Alymbaeva DB, Zamiatina NA, Dzhumalieva DI, et al. Further study of experimental hepatitis E in piglets. Vopr Virusol 1994; 39: 208-12.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: