
Mohammad Golshan ( Department of Paediatric, Shahid Sadoughi University of Medical Sciences and Health Services, Yazd, Iran. )
Nematizadeh Hossein ( Department of Paediatric, Shahid Sadoughi University of Medical Sciences and Health Services, Yazd, Iran. )
September 2013, Volume 63, Issue 9
Original Article
Abstract
Objective: To compare the extraction time and infection rate of umbilical cord by applying ethanol, humanmilk or dry care.
Method: The parallel single-blinded randomised clinical trial was performed on 300 neonates at Shahid Sadougi University of Medical Sciences and Health Service, Yazd, Iran, between March and September 2010. The neonates were divided into three random but numerically equal groups. Each group was assigned the application of ethanol or mother’s milk or to keep the stump dry. The neonates were visited on the 3rd and the 7th day after birth and follow-up was maintained telephonically until umbilical separation. Umbilical separation time and umbilical local infection frequency were considered as the study outcome, which was compared among the three groups according to age, gender and delivery type of the neonates.
Results: Umbilical separation time in neonates of the human milk group had significant difference with the ethanol group (p=0.0001) and drying groups (p=0.003). Frequency of omphalitis had no significant difference among the three groups.
Conclusion: Topical usage of human milk on umbilical cord stamp decreased separation time and incidence rate of omphalitis.
Keywords: Umbilical cord, Human milk, Ethanol, Dry care, Separation time. (JPMA 63: 1117; 2013).
Introduction
One million neonates die due to umbilical cord infection. Most of these mortalities occurr in developing countries. According to a recent World Health Organisation (WHO) report 300,000 neonates die annually due to tetanus infection, and umbilical cord is the leading route for such an infection.1,2
Umbilical cords converts into necrotic tissue and becomes a suitable media for infection pathogens in the environment. Staphylococcus aureus, Escherichia coli and streptococcus in group B are common pathogens.1 Using anti-bacterial treatments in neonatal umbilical cord are associated with lower bacterial penetration, but reduce leukocytes secretion which are needed for umbilical cord extraction. Delay in the extraction can increase umbilical infection.1,3 According to complications related to different methods of extraction, WHO recommended drying of umbilical cord as a suitable method. Though several studies have supported this recommendation,1,4 there are contradictory statements about this method as well.2
Human breast milk is considered a better management practice and is used in some countries.2 Human milk can accelerate complex umbilical extraction according to its leukocytes or polymorphonuclear cells. Neonates who used human milk had lower umbilical extraction time compared to those who used antiseptic solutions.2 The present randomised clinical trial was conducted to compare the impact of three therapeutic methods human milk, drying and ethanol 70% on the separation of umbilical cord.
Patients and Methods
During the study period between March and September 2010, all healthy term (37-42 weeks) neonates (n=316) were included in the trial at Shahid Sadoughi Hospital of Shahid Sadoughi University of Medical Sciences and Health Services. The study was approved by the institutional ethics committee, and informed consent was obtained from the parents of each neonate. The inclusion criteria comprised neonates who were delivered with normal vaginal or Caesarean section and healthy term neonates with 37-42 weeks gestational age and without other medical complications or disorders such as maternal abnormalities or respiratory distress, asphyxia, or metabolic disorders. Age, gender, delivery type and complications were recorded in the checklist.
The neonates were divided into three groups [ethanol topical human milk] randomly with the help of the numbers table. Age and gender of the neonates were matched. In the ethanol group, mothers washed the umbilical stump with 70% ethanol two times a day for two days after umbilical separation. In the milk group, mothers washed the umbilical cord stump with their milk two times a day for two days after umbilical separation. In the third group, mothers only dried the umbilical stump until umbilical separation. Neonates were visited on the 3rd and the 7th day in hospital after birth, and were followed up through telephone after one week until umbilical separation. Neonates whose umbilical cords were not separated during the first week of life were followed up until its separation. Omphalitis symptoms, such as infectious discharge or circular erythema or rigidity around the umbilicus or in the anterior of the abdomen, were kept an eye on. Umbilical separation time and umbilical local infection frequency were considered as the study outcome, which was compared among the three groups according to age, gender and delivery type of the neonates.
Data was analyzed through SPSS 16. Quantitative variables were presented as mean and standard deviation, while qualitative variables were presented as frequency and percentage. Umbilical separation time was taken as quantitative, and frequency of omphalitis as a qualitative variable among the neonates of the three groups for the purpose of Fisher Exact test and analysis of variance (ANOVA) tests. Two-tailed significance level of 0.05 was used to detect difference between the variables.
Results
The initial Primary study population was 316, but 16(5.06%) neonates had to be excluded: 10(3.16%) for not meeting the eligibility criteria or parents declined to participate. The final sample size as such 300. In the assessment of basic variables, none had significant difference among the three groups. The mean of maternal age, number of pregnancies neonatal weight and gestational age also had no significant differences, (Table-1).
The mean of umbilical separation time had significant differences among the three groups (p <0.0001). The lowest and the highest separation times belonged to human milk and ethanol groups respectively. Among the neonates, the lowest and the highest umbilicus separation times were 3 and 15 days. In post hoc analysis, umbilical separation time in human milk group had significant differences with ethanol (p <0.0001) and drying groups (p <0.003), (Table-2).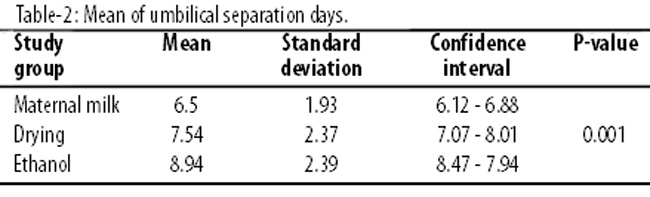
The frequency of omphalitis did not have significant differences among the three groups. We had only 1(1%) neonate in the drying group and 2(2%) neonates in the ethanol group, while there was none in the human milk group with omphalitis. Mothers of 4(4%) neonates in the human milk group, 3(3%) neonates in the ethanol group and 3(3%) neonates in the drying group were using antibiotics. There were no significant differences among the three groups, on this count.
Discussion
The present study showed that the mean of umbilical separation time had significant difference among the three groups. Umbilical separation time in neonates of the human milk group had significant differences with the other two groups. A study on 312 neonates who received ethyl alcohol, human milk, silver sulfadiazine and drying method for clearing and drying of the umbilical cord, reported that the mean of separation time in the human milk group was significantly lower than the other groups, and increased respectively in alcohol, drying and silver sulfadiazine groups. Omphalitis was not seen in any of the neonates.3
Another study on 77 neonates reported that Escherichia coli and Streptococcus group B colonisation in the umbilical cord stamp in neonates who received drying was significantly higher than those who received ethanol 70%. The mean of umbilical cord separating time had no significant difference between the two groups.5 A study on 118 neonates in two groups of human milk and drying for colonisation of pathogen and non-pathogen organisms showed that pathogen organisms colonised significantly lower in neonates who received topical human milk in their umbilical cord against the non-pathogen organisms. The mean of separation time of the umbilical cord was significantly lower in neonates with topical human milk.1 In the light of to above studies, it seems that in developing countries, health policy of umbilical cord drying needs more assessments.
According to WHO recommendations, some factors like topical antiseptic usage, infection and Cesarean section were responsible for delaying umbilical cord separation.6 Topical antiseptic usage on the stump of umbilical cord reduced bacterial colonisation and leukocytes secretion, which were necessary for umbilical cord separation, and increased the infection rate.1,3 Several hospital-based studies for alcohol usage in umbilical cord cleaning showed that alcohol had lower impact on infection rate and bacterial colonisation on umbilical cord stump compared to other antiseptic solutions such as Triple-Day and Chlorhexidine.7 Alcohol delayed umbilical cord separation and in some neonates who used alcohol for over 21 days for umbilical cord cleaning, toxicity symptoms such as haemorrhage, skin necrosis, central nervous system impairment and hypoglycaemia might occur.7,8
Umbilical cord separation is a complicated process and histological studies have reported polymorphonuclear infiltration between the umbilical cord stump and the abdominal wall. Human milk accelerates umbilical cord separation process because it has polymorphonuclear and photolytic enzymes.3
Conclusion
The use of human milk as topical therapy can decrease separation time in neonates compared other methods. This can be used as a suitable, safe and non-expensive method for umbilical cord management.
References
1. Taffazoli M, Farahani LA, Mohammadzadeh A, Esmaeeli H, Ghazvini K. Dose topical application of breast milk affect on bactrial colonization in umblical cord? J Semnan Uni Med Sci 2008; 10: 29-35.
2. Vural G, Kiza S. Umblical cord care: a pilot study comparing topical human milk, povidone-iodine and dry care. J Obster Gynecol Neonatal Nurse 2006; 35: 123-8.
3. Ahmadpour-Kacho M, Zahedpasha Y, Hajian K, Javadi J, Talebian H. The effect of topical application of human milk, ethylalcohol 96% and silver sulfadiazin on umblical cord separation time in newborn infant. Arch Iranian Med 2006; 9: 33-8.
4. McInerny T, Adam HM, Campbell DE, Kamat DM, Kelleher KJ (eds.). American Academy of Pediatrics: Textbook of Pediatric Care. 5th edition. America: American Academy of Pediatrics; 2009.
5. Nourian M, Allaii F, Heidari A. Comparison of the effect of alcohol 70% versus dry cord care on cord bacterial colonization and cord separation time among newborns. Pak J Med Sci 2009; 25: 103-7.
6. World Health Organization. Post partum care of the mother and newborn, care of the umblical cord. 1998 (Online) (Cited 2010 June 10). Available from URL: http://www.who.int/reproductivehealth/publication.
7. Darmstadt G, Dinulos J. Neonatal skin care. Pediatr Clin North Am 2000; 47: 757-82.
8. Spray A, Siegfried E. Dermatologic toxicology in children. Pediatr Ann 2001; 30: 197-202.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: