
Zulfiqar Ahmed Bhutta ( Department of Neonatal Services, The Aga Khan University, Karachi. )
March 1995, Volume 45, Issue 3
Original Article
Abstract
Primary ciliary dyskinesia (PCD) is a rare disorder associated with chronic respiratory problems and even more infrequently as a cause of neonatal respiratory distress. Of consecutive 12 children seen with a diagnosis of PCD, the disorder presented within the neonatal period in 11, with a positive family history in 50%. The diagnosis was delayed in several cases, despite suggestive radiological findings. The data highlights the importance of recognizing PCD in newborns presenting with early respiratory distress and isolated dextrocardia (JPMA 45: 70, 1995).
Introduction
Respiratory distress in the newborn period is a common mode of presentation of a variety of pulmonary and extra pulmonary disorders. While surfactant deficiency respiratory distress syndrome heads the list in premature infants, a number of other problems may also lead to respiratory distress in term infants and include diverse disorders such as pulmonary maladaptation. congenital pneumonia, meconium aspiration syndrome, metabolic disorders and persistent pulmonary hypertension. Primary abnormalities of ciliary function have been recognized as a cause of chronic respiratory problems in childhood and adult life in recent years1. With the chance discovery of abnormalities of spermatozoal motility in such individuals2, a pathophysiological basis for this disorder, labelled immotile cilia syndrome, became known3. The disorder represents a heterogenous group of abnormalities ranging from complete ciliary immotility to diverse ultrastmctural and functional derangements leading to altered mucociliary clearance and more appropriately called pnmaiy ciliaiy dyskinesia (PCD) 4. The clinical presentation of PCD varies greatly, with most patients becoming symptomatic in early childhood and some in the neonatal period1. In the first systematic description of the disorder in the newborn period, Whitelaw et al described six neonates with severe respiratory distress due to ciliary dysfunction5 and emphasized the importance of prompt recognition and initiation of therapy within the neonatal period. As ultrastructumi and functional ciliaiy studies may be difficult in the neonatal period, the diagnosis may need to be made oh clinical grounds. In particular, although a significant proportion of patients with PCD may have situs solitus, the association of situs inversus with respiratory problems in the neonatal period are highly suggestive of the disorder. We present a consecutive series of infants presenting to the Aga Khan University Hospital (AKUH) with features consistent with a diagnosis of PCD.
Patients and Methods
Over a seven year period (1987-1993), 12 children presented to the AKUH with features consistent with a diagnosis of PCD. These consisted of situs inversus, respiratory difficulty and recurrent bouts of wheezing and pneumonia. Since facilities for ultrastmctural examination and ciliary functional studies were not available in Pakistan, the diagnosis in all but one was based on clinical criteria and exclusion of other causes of recurrent respiratory problems such as reactive airways disease, immunodeficiency and cystic fibrosis.
Results
The clinical characteristics of these children are presented in Table I.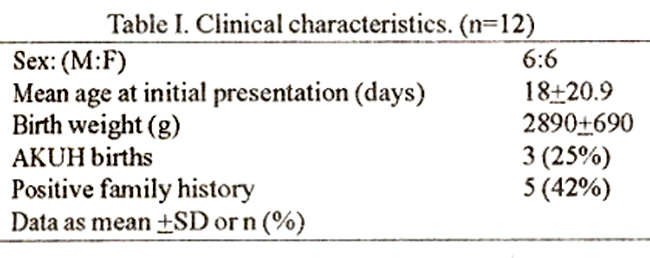
The age at presentation ranged from 1-84 days. Although 6 presented to the hospital after the neonatal period, in nearly all cases symptoms developed within the neonatal period, in some immediately afterbirth Two children remained well afterbirth but developed symptoms of respiratory difficulty by three and twelve weeks of age respectively. Majority (9/12) were referred from outside hospitals, whereas three were born at AKUH, giving an incidence of 0.6 per thousand AKUH births for this period. A family histoiy of recurrent respiratory problems and/or sibling death was discernible in only 6 cases (50%). The clinical features at presentation in the cohort are given in Table II.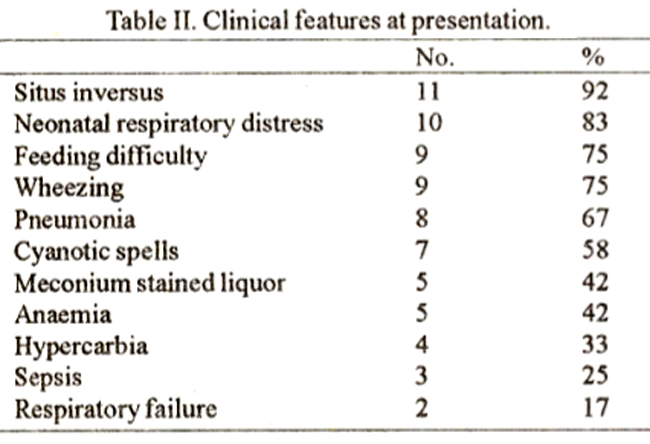
Majority 10/12 (83%) presented with features of respiratory distress and feeding difficulty within 24-48 hours after birth. In 5 (42%) there was a clear history of meconium passage inutero and 7(58%) had cyanotic spells as a prominent feature at presentation. Two neonates, including one born at AKUH, developed signs of respiratory failure and severe distress within 24 hours of admission, necessitating artificial ventilation and intensive respiratory support. In only one of the 9 patients referred from outside, was a diagnosis of PCD entertained at any stage. The commonest provisional diagnosis among the neonatal referrals was congenital heart disease, followed by congenital pneumonia, whereas older children were treated for a variety of disorders including tuberculosis, asthma, suspected immune deficiency etc. Investigations of the neonates at admission included a chest X- ray, hematological profile and blood gas analysis. Situs inversus was documented in 11/12(92%). Radiological evidence of atelectasis/pneumonia was seen in 8/12 (67%), whereas two older children presented with clinical and radiological features of bronchiectasis. The sinuses were X-rayed in three of the older children and revealed abnormalities and opaciuication in all. Significant anaemia necessitating blood transfusion was seen in 4/12 (33%). Four infants had clinical evidence of sepsis at admission and therefore. received broad spectrum antibiotic therapy. Blood cultures revealed Enterobacter cloacae and Pseudomonas aeruginosa in two neonates. Significant hypercarbia was noted in three infants at admission but only two of these required a brief period of assisted ventilation (2 and 4 days respectively). Two neonates also underwent echocardiography for persistent cyanosis, of whom one was documented to have a congenitally corrected transposition of great vessels. The diagnosis of PCD was based on clinical criteria as radiological findings as ultrastructural studies were not available locally and the saccharin test was impractical in the age group. A nasal mucosal biopsy from one patient however, was hand carried by the father in glutaraldehyde for electron microscopy to Riyadh, which confirmed the absence of outer dynein arms in the cilia studied (Figure).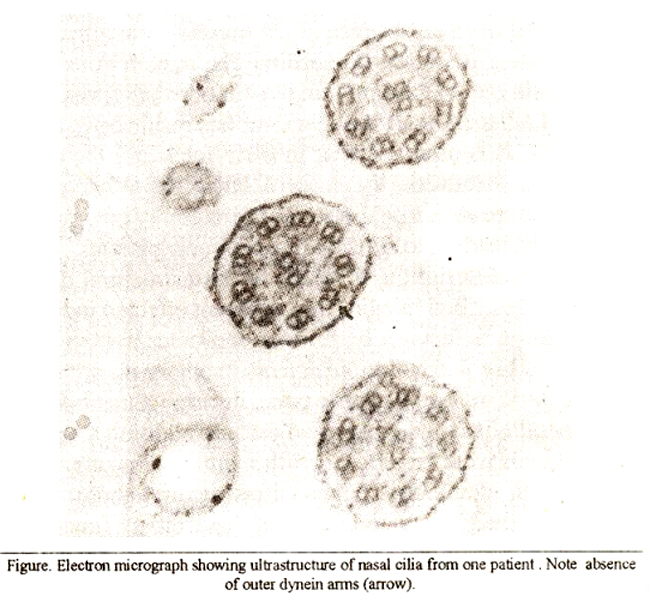
The one newborn with recurrent atelectasis and situs solitus, had a normal immunoglobulin profile and sweat chloride levels. There were no deaths during the course of hospitalization. All children were placed on a regimen of strict physiotherapy and postural drainage. Inhaled and oral bronchodilator therapy with salbutamol was administered as necessary. In all, follow-up data upto 5 years was available in 10/12 children. Although the short term follow-up was satisfactory, long term compliance and adherence to a strict regime of regular physiotherapy and postural drainage was poor and 3 neonates failed to return for an extended period of time. Several also underwent alternative form of therapy e.g., homeopathy for varying periods of time. Despite full instructions on diagnosis and therapy, one child’s parents moved to another city where therapy was stopped at the “advice” of the family physician. The child returned three years later with features ofbronchiectasis. Two children were lost to follow-up. The girl with congenitally corrected transposition remains well. Table III details the various complications encountered during the course of therapy and follow-up in the cohort. Recurrent episodes of wheezing and pneumonia were the commonest complications requiring medical therapy and repeated hospitalizations.
Discussion
Original studies of immotile cilia syndrome indicated that the disorder was inherited in an autosomal recessive form and resulted from an absence of the outer dynein arms in the cilia, resulting in ciliary immotility. The dynein arms of the cilia contain the ATPase pmtein dynein which induces active sliding of adjacent microtubular doublets resulting in ciiaty movement. It is assumed that in early fetal life, the ciliaiy movements determine the type of laterality. When ciliaty movements are absent or abnormal, the lateralit may develop fortuitously, leading to situs inversus in some patients6. Since this original description, a variety of ultrastructural defects have been described in cilia from different effected individuals, including defects in both inner and outer dynein arms, absent radial spokes. multiple defects in ciliary microtubules e.g., eccentric or absent centric pairs, disarrangement, loss of ciliary parallelism and compound cilia. In addition a number of individuals were recognized with a similar clinical presentation but no identifiable ciliai ultrastructural abnormality. These individuals were considered to have ciliary functional abnormalities resulting in altered mucociliary clearance. It is thus apparent that the syndrome represents a heterogenous mixture of disorders, ranging from minor afflictions to severe life threatening forms of the disorders. Therefore, Sleigh et al4 proposed the term primary ciliary dyskinesia (PCD) as abetter description of the range of ciliary abnormalities. Although symptoms may start during early childhood, the diagnosis is frequently missed and symptomatic treatment for recurrent bouts of wheezing and lower respiratory infections is offered in most cases. The disorder may become clinically evident, as in tho majority of our cases, by the concomitant presence of situs inversus. With normal situs however, the diagnosis is fairly difficult unless sophisticated tests for ciliaiy ultrastructure or function are carried out. Although the saccharin test offers a simple screening test in adults, it is of limited value inearly childhood. The description of a quantitative estimate of ciliary beat frequency and motility (1980), offered the possibility of a screening test for ciliary function in infancy7,8. A major limitation of ciliary screening tests however, is the observation that ciliaiy ultrastructural and microtubular
abnormalities may result fmm intercurrent viral or punilent infections9,10. Wilson et al also demonstrated reduced ciliary beat frequency from sites of purulent infection11 and it was shown that serine proteinase from sites of inflammation also reduced ciliaty beat frequency12. Thus in a situation where there is coexistent infection, minor degrees of ciliary dyskinesia may be difficult to interpret. These latter observations, coupled with the limited availability of functional investigations even in research facilities indicate that in most patients the diagnosis is based on a highly suggestive clinical picture and exclusion of alternative diagnose. While the primary manifestation of PCD in children is with resFiratorv problems13, other atypical presentations are known14,15. An association of PCD with defects in neutrophil chemotaxis16,17 is well described. While we do not have information on neutrophi! motility in our patients, 2/16(33%) of our patients presenting in the neonatal period, had concomitant bacterial sepsis. It is not uncommon for symptoms to become manifest in the neonatal period. In the series by Greenstone et al1, 44% of the patients gave a history of respiratory problems in the perinatal period. According to Buchdahl et al18 a history of onset of symptoms in the neonatal period in children with chronic respiratory problems is strongly suggestive of ciliaiy dysfunctions. The disorder is strongly suggested by the presence of situs inversus, but this may not invariably present19. Although nearly all the children in our series had situs inversus, we feel that this may represent an under diagnosis of the disorder in other children with recurrent respirabory problems and normal situs. Recent series in adults have pointed out the presence of the disorder in the Pakistani population20, and with the high incidence of consanguinity in ourpopulation, it is likely thata large numberof suchcases are being missed. Although isolated cases of PCD had been described in neonates, Whitelaw et al5 were the first to emphasize the potential of PCD in newborn infants with respiratory distress. In our series, a history of respiratory distress after birth was evident in almost all patients referred from outside, but despite the evidence ofsitus inversus, the diagnosis had not been made in the neonatal period. Our data suggests the neonatals presentation of PCD is common among patients who are severely afflicted. The disorder should therefore be considered in every newborn with unexplained respiratory distress and recurrent atelectasis and is highly suggested by the presence of situs inversus. It is important to make the diagnosis early, as regular physiotherapy and postural drainage may prevent the inexorable respiratory infections and progression to bronchiectasis.
Acknowledgement
We are grateful to Dr. M. Akhtar of the King Faisal Specialist Hospital and Research Center, Riyadh for the ultrastructural evaluation of nasal mucosa in our patients.
References
1. Greenstonc, M., Rutman, A., Dewar, A. et at. Primary cihaiy dyskinesia: cytological and clinical features. Q. J. Med., 1988;253:405-30.
2. Pederson, H. and Rebbe, H. Absence of arms in the axoneme of immunowhile human spermatozoa. Bio Reprod., 1975; 12:541-4.
3, Eliasson, R., Mosseberg, B., Camner, P. et at. The immotile-Cilia Syndrome. N. Engi. J. Med., 1977;297:1-6.
4. Sleigh, M.A. Primary ciliary dyskinesia (Letter), Lancet, 1981 ;ii:476.
5. Whitelaw, A., Evan, A. and Corrin, B. Immotile Cilia Syndrome: a new cause of neonatal respiratory distress. Arch. Dis. Child., 1981;56:432-35.
6. Friday, GA., Yunis, E.J. and Agostini, R.M. Immotile Cilia Syndrome. Pediatr. Clin. North Am., 1981;28:807-12.
7. Greenstone, MA., Jones, R.W.A., Dewar, A. et at. Hydrocephalus and primary ciliary dyskinesia. Arch. Dis. Child., 1984;59:481-2.
8. Rutland, J. and Cole, P.J. Non-invasive sampling ofnasal cilia formeasurement of beat frequency and study ofultrastructure. Lancet, 1980;ii:564-5.
9. Corebeel, L., Comiltie, F, Lauweiyns, J. et at. Ultrastructural abnormalities of bronchial cilia in children with recurrent airway infections and bronchiectasis. Arch. Dis. Child., 1981;56:929-33.
10. Carson, J.L., Collier, AM. and Shih-Chin, S. Acquired ciliary defects in nasal epithelium of children with acute viral upper respiratory infections. N. EngI. J. Med., 1985;312:463-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: