
Abdul Baqi Durrani ( Departments of Medicine and Paediatrics, Bolan Medical College, Quetta. )
Ismat Ullah Durrani ( Departments of Medicine and Paediatrics, Bolan Medical College, Quetta. )
Nighat Abbas ( Departments of Medicine and Paediatrics, Bolan Medical College, Quetta. )
Munawar Jabeen ( Departments of Medicine and Paediatrics, Bolan Medical College, Quetta. )
August 1997, Volume 47, Issue 8
Original Article
Abstract
Over the past 5 years, 1620 comatosed patients of both sexes aged 1-75 years were screened for cerebral malaria. Of these, 505 (31.2%) were positive for Plasmodium falciparum. During this period frequency of malaria increased from 22.1% in 1991 to 44.4% in 1995. Sixty-four percent cases of cerebral malaria were seen in children and thirty-six percent in adults. Mortality was also higher (41%) in children than in adults (25%). As cerebral malaria is particularly prevalent in Pakistan and is a major conununity problem, accurate and easier methods of its diagnosis are needed at primary health care level, in all febrile comatose patients, without focal neurological findings. (JPMA 47:213,1997).
Introduction
Cerebral malaria is associated with increased mortality in endemic areas, especially in children1, Most deaths occur within 3 days of admission. Altered consciousness in presence of P. falciparum must be taken as a clinical indication of cerebral malaria. Convulsions occur in children and adults. Neck rigidity is not afeature, althoughmild neck stiffness may be present Raised intracranial pressure is not seen in cerebral malaria. Focal neurological signs are uncommon. Severe malaria is defmed parasitologically as over 5% of red cells parasitised, although complicated malaria can occurwith only 1% of red cells parasitised; clinical assessment is therefore very important. The major differential diagnoses include meningitis, meningoencephalitis and delirium commonly found with high grade fever2. This study reports a gradual increase inthe prevalence of cerebral malaria overthe last five years.
Patients and Methods
To determine the frequency and mortality of cerebral malaria, all febrile patients admitted to medical and paediatric units of Jinnah Post graduate Medical Centre (JPMC),Karachi (1000) and Sandeman Provincial Hospital, Quetta (620) from January, 1991 to December, 1995 with drowsiness, headache, psychosis, delirium, hallucinations or seizures pmgressing to coma with their blood smears positive for Plasmodiuin ring stage or trophozoites were included in this study. Eighty-one of these cases had jaundice.
Investigations included thick and thin blood smears for malarial parasites and analysis of cerebrospinal fluid. Ten consecutive fields of thick blood films stained with giemsa stain were examined under a microscope with a magnification of X 100 for malarial parasites. Blood smears of all patients with cerebral malaria were positive for P. falciparum with nng stage trophozoites and cerebrospinal fluid analysis was normal. All of 81 icteric patients in this study had negative viral serology. Blood culture done in 29 patients was negative. Investigations were done in Basic Medical Sciences Institute, JPMC, The Lab, Aga Khan University Hospital Laboratory in Karachi and Diagnostic Laboratoty, Fayaz Lab and Clinical Laboratory of Sandeman Provincial Hospital in Quetta.
Results
A total of 1620 febrile cases of both sexes, progressing to coma were screened. Fifty percent patients with cerebral malaria were children between 0 to 15 years and 19% were adults (Figure 1).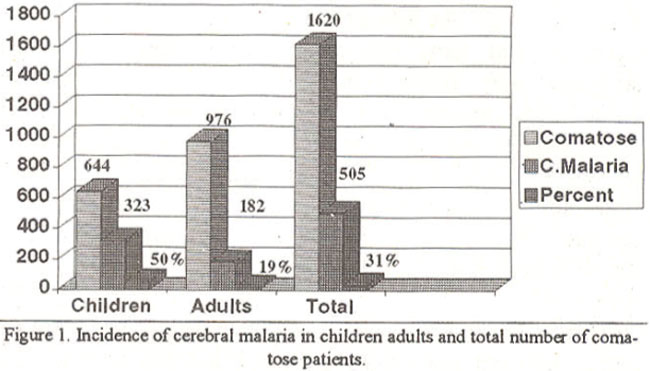
Thirty one percent (505), febnle comatose patients including 264 males and 241 females, had cerebral malaria.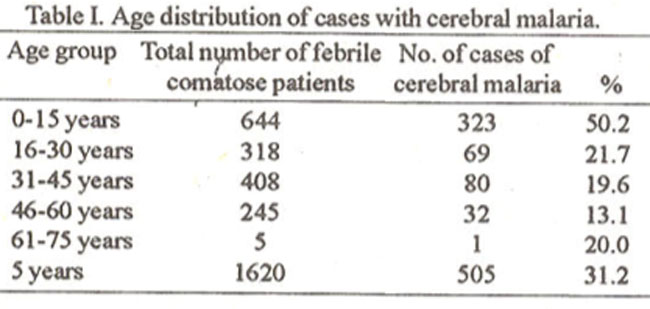
Table I shows the age distribution of these cases. A rise in the frequency of cerebral malaria was seen over the last 5 years. The yearwise distribution is given in Table II.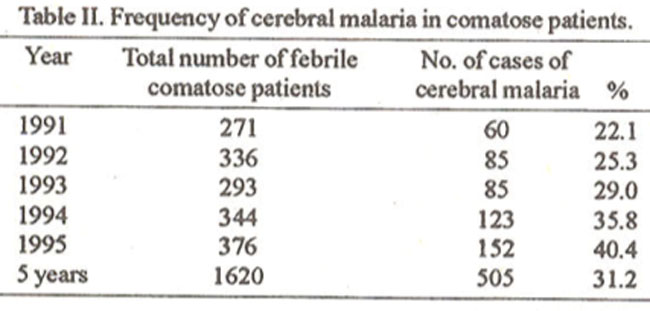
No significant difference was seen in the incidence of cerebral malaria, in Karachi and Quetta (Table III).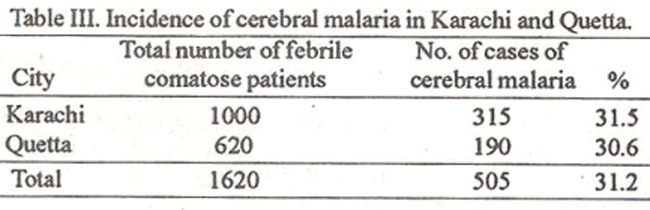
The highest mortality was seen in children as given in Figure 2,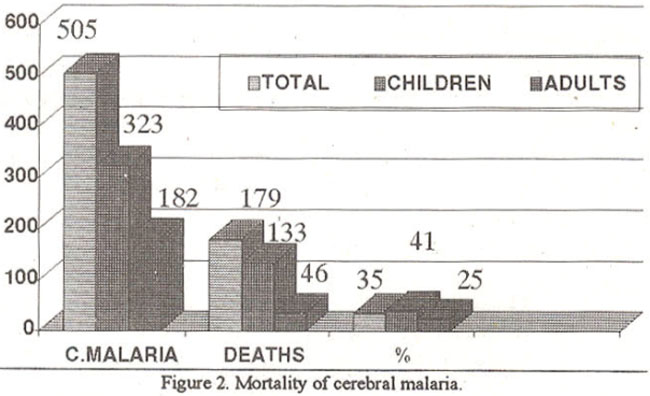
whichalso illustrates the mortality in adults and total number of patients with cerebral malaria.
More than five million cases of nialaria are reported annually from countries south of Sahara. About 75% of these cases are from 9 countries including India3. Although, Pakistan is not included in this group, but malaria is endemic in this country. Falciparum malaria is seen with vaiying presentations including cerebral malaria and fulminant hepatic failure4,5. Cerebral malaria is the most important complication of falciparum, being the predominant species of Plasmodium in the last decade6. During the five years study the frequency of cerebral malaria in febrile comatose patients ranged from 22.1% to 40.4% with a gradual increase from 1991 to 1995. Although children account for 50% of cerebral malaria, the frequency has also increased in adults. The general increase infrequency is very alarming. If this persists thenwe would be facing a very complicated situation. Ourlife style, low literacy, geographical location, inigation and agricultural methods encourage standing pools of water, all contribute to this situation. Cerebral malaria canies a very high mortality and morbidity6,7,8. To prevent the general increase in frequency and thus decreasing the mortality, new strategies for its control are needed. Early diagnosis and effective treatment should be the main contml measure in this situation. Impregnated bednets may also be helpful.
References
1. Carme, B.. Yombi. B.. Bouquety, J.C. et al. Child morbidity due to cerebral malaria in Brazzaville. Imp. Med. Parasitol., 1992;43:173-76.
2. Wright, P.W., Avery, W.C., Ardill, WD. etal Ininal clinical asscssnent of the comatose patients: Car ebral malaia vs meningitis Pediatt Infect Dis. J., 1993;12:37-41.
3. World malaria situation 1990. Division of control of tropical diseases. World Health Organization, Geneva, World Health Stat. Q., 1992,45:257-266.
4. Ahsan, T., Rab, S.M. and Shekhani, MS. Falciparum malaria or fulminant hepatic failure? J. Pak. Med. Assoc., 1993;43:206-208.
5. Joshi, YK., Tandon, BK., Archarya, S.K. et al. Acute hepatic failure due to plasmodium falciparum liver injury. Liver, 1986;6:357.360.
6. Rafi, S., Memon, MA.. Rao, M.H. et al. A change of Plasmodium species in fecting children in Karachi over the last decade. J. Pak. Med. Assoc.. 1994;44: 162-164.
7. Brewster, D.R. and Kwiatkosi-White, N.J. Neurological sequelae of cerebral malaria in children. Lancet, 1990;ii: 1039-43.
8. Richter, R.W. Infections other than AIDS. Neurol. Clin., 1993;11:591-603.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: