
Aliya B. Aziz ( Departments of Obstetrics, Aga Khan University Hospital, Karachi. )
Saeed Hamid ( Departments of Gynaecology and Medicines, Aga Khan University Hospital, Karachi. )
Saima Iqbal ( Departments of Gynaecology and Medicines, Aga Khan University Hospital, Karachi. )
Wahila Islam ( Departments of Gynaecology and Medicines, Aga Khan University Hospital, Karachi. )
Sadia Aziz Karim ( Departments of Obstetrics, Aga Khan University Hospital, Karachi. )
August 1997, Volume 47, Issue 8
Original Article
Abstract
A hospital based observational study was carried out on pregnant women presenting with either acute hepatitis or fulminant hepatic failure (FHF), during the past years. Of 53 patients, 20 (38%) developed FHF.Non-A, Non-B was the commonest cause (62%) followed by hepatitis B in 17% and hepatitis A in 4% cases. Eight women expired (case fatality rate 15%) with a high maternal mortality (62%) caused by NANB hepatitis. Perinatal mortality was 30%. Poor prognostic factors identified were lack of antenatal care, severity of jaundice, history of somnolence, gastrointestinal bleeding and a high grade of encephalopathy (JPMA 47:198,1997).
Introduction
Hepatitis in pregnancy presents challenging questions to the obstetrician. Most Asian countries have a highbirth rate and a large pool of hepatotropic viruses causing hepatitis in pregnancy1. Pakistan is endemic for all types of hepatitis2 and bothepidemic3 and sporadic forms have been reported4. Of the 5 viruses known to cause viral hepatitis A and E are water-borne agents, the infection being usually acquired by drinking fecally contaminated water.Both these agents are highly endemic in this region. This study was conducted to identify the relative frequency of various hepatotmpic viruses causing acute heçatitis in pregnant women, their clinical presentations, effects on pregnancy and the risk factors for severe, life threatening viral hepatitis in pregnancy.
Patients and Methods
This study was carried out on the pregnant women admitted in Internal Medicine or Obstetrics and Gynaecology departments of the Aga Khan University Medical Centre during the past 5 years (January, 1990 to December, 1994).
These patients fulfilled the following criteria for either acute viral hepatitis or fulminant hepatic failure caused by viral hepatitis.
Criteria for diagnosing acute viral hepatitis were:
1. Recent onset ofjaundice.
2. No othercause accountable forjaundice e.g.,pre-eclampsia, eclampsia, cholestasis of pregnancy, severe infections, drugs etc. excluded on the basis of histoiy, physical exanunationand laboratory tests.
3. Serum transaminase levels atleast more than three times normal (0-55 iu/I).
Criteria for diagnosing severe/fulminant hepatitis were:
4.Theabovementionedparametersfotthediagnosisofacute viral hepatitis plus
5. Presence of hepatic encephalopathy and
6. Prulonged prothrombin time to more than four seconds of control.
Hepatic encephalopathy was gmdedfrom 1-4 according to the definitions proposed by Trey and Davidson5. The study had 2 parts, one retrospective in which all those patients who were admitted with the above mentioned diagnoses during a 3 year period, from January, 1990 - December, 1992, were identified and included in the study. These patients were identified by the indexing and coding unit of the medical records departinent of the Aga Khan University Hospital. This unit obtained records of the above mentioned cases from the medical records with the help of lCD 9 CM classified system (international classification of diseases 9th revision, clinical modification). The second part of the study was a 2 year prospective study from January 1993 - December 1994, during which all patients presenting withthe above mentioned criteria were included. A questionnaire was filled for each patient which covered personal and demographic data including household, social and environmental factors and potential risk factors for the acquistion of viral hepatitis. The data was collected under categories of general data of patient including age, parity, presence of risk factors, obstetric data including past pregnancies, antenatal care, HBsAg screening and data regarding present illness like gestational age at the onset of illness, signs and symptoms, days to progression to hepatic encephalopathy and grades of encephalopathy.
Laboratory investigations included levels of total, direct and indirect bilirubin aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma GT (GGT) and serum alkaline phosphatase (SAP) were determined. Total serum proteins and levels of albunun and globulin were also determined. Renal function tests, uric acid and complete blood picture with a IgG) was performed by a newly developed EIA method at CDC Atlanta, USA (H. Fields, manuscript in preparation).
Patients were followed-up after the acute phase was over in Medicine and Obstetrics clinics. Autopsy was not performed for abortus or after still biiths and neonatal deaths.
Only one patient agreed fora liver biopsy.
Data analysis
Data was entered on EPI-INFO version 5.0 and final statistical analysis was done with the help of statistical package SPSS for windows.
Results
During the 5 year study period, a total of 53 pregnant women were admitted with the diagnosis of acute viral hepatitis (AVH) and of these 20, were in the fulminant hepatic None of the women diagnosed as hepatitis A developed FHF.
Majority of women belonging to all etiologic groups, except hepatitis A, presented inthe 2nd or 3rd trimester while both the women with hepatitis A presented in the 1st trimester. Eight women expired, of these, 5 had NANB hepatitis, 2 had hepatitis B and belonged to undefined group. Case fatality rate was 15%. Socio-economic class, mean age and other demographic data were comparable in four different eliologic groups, although the mean parity (5.3) was significantly higher in patients infected with HBV as compared to those infected with HAV (2.5) or NANB (2.7), (P value= .005).
Comparison of clinical features revealed that 65.2% patients presenting with moderate (bilirubin >10 mg/dl) and 82.4% of those presenting with severe jaundice (biirubin >15 mg/dl) were infected by NANB virus. The mean serum transaminase and alkaline phosphatase were comparable among the four failure (FHF) or developed it during the hospitalization. During this period a total of 8940 obstetric patients were admitted and therefore, the prevalence of acute viral hepatitis among the obstetric related admissions was 0.59%. The prevalence of FHF out of acute viral hepatitis was 38% (20 out of 53). The NANB viruses were the cause in 34(64%) cases followed hepatitis B virus in 9(17%) and hepatitis A virus in2 (4%) cases. In 8 cases complete serology was not performed and they were classified as undefined group. No case of acute hepatitis C was detected and none of the hepatitis B patients were positive for the Delta virus. Further serological analysis of 25 of the 34 cases belonging to the NANB group was done for hepatitis C and hepatitis E. The remaining 9 patients could not be tested as they belonged to the retrospective part of the study. Hepatitis E virus was detected in 8 out of 12 cases tested. In addition to these, 13 cases were also screened for hepatitis C virus and as they were found non-reactive for C virus they were grouped under NANBNC. This group by diagnosis of exclusion could also be taken as hepatitis E, making a total of 21 cases comprising of 62% of the NANB group and 40% of the total cases.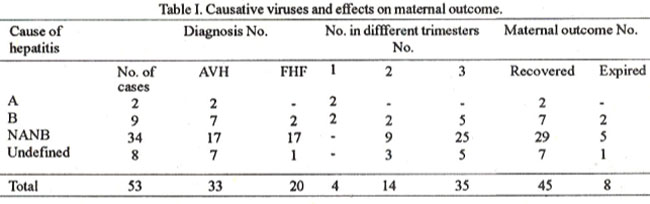
Table I shows viral etiologic groups, their trimester of presentation, numberpmgressing to FHF and the maternal outcome. Half of those diagnosed as NANB progressed to FHF as comapred to only 22% and 12.5% in the hepatitis B and undefined group respectively.
groups but serum bilirubin was significantly lower in those affected by hepatitis A.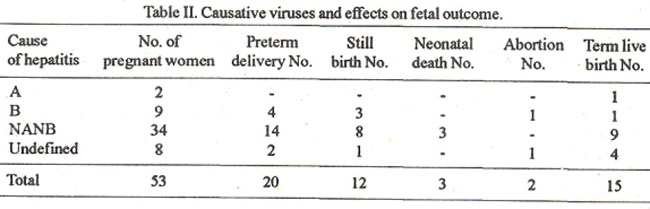
Table II shows the fetal outcome in the different groups.Most of the pretenn deliveries (14 of 20), still births (8 of 12) and neonatal deaths (3 of 3) occurred inpatients infected with NANB hepatitis. One patient suffering from hepatitis A was lost to follow-up. Perinatal mortality was 3O%. Comparison of different clinical parameters observed inFHF and non-FHF patients is shown in Table III.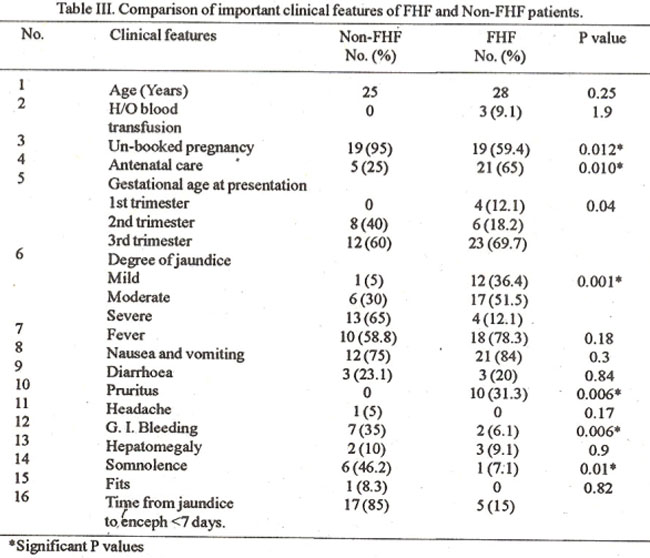
Afull description of 12 of the FHF patients is reported elsewhere6. There was no significant difference in mean ages among the two groups.
Among the FHF patients, 95% were not booked at our institution as compared to 59.4% of the non- fulminant patients. In the FHF group, 65% of the women presented with severe jaundice in comparison to only 12% in the nonfuhuinant group. Gastrointestinal bleeding was observed in 35% patients with FHF as compared to only in 6.1% of non-fulminant patients. A history of somnolence was significant in the FHF cases (46%). Majority of FHF patients belonged to the lower middle and low socioeconomic classes.
Majority of patients in FHF had an interval between jaundice and encephalopathy of<7 days while in non-fuhninant group veiy few had this kind of rapid progression. Comparison of laboratory parameters among FHF and non-VHF patients revealed that the mean senim biirubin level was significantly high in the patients with FHF (19.2 mg/dl versus 8.2 mg/dl). Prothrombin thue and A.P.T.T were also significantly deranged inthe FHF group as were BUN and creatinine levels, suggestive of the presence of coagulopathy and hepatorenal syndrome in VHF patients. Maternal and fetal outcome revealed that all 8 mortalities were in FHF group and rates of stillbirths (9 versus 3) and pretemi delivery (11 versus 9) was also significantly higher in FHF patients. When the same clinical and laboratory parameters were compared among the fatal and non-fatal cases of FHF, the only factor of prognostic significance was the grade of encephalopathy. All patients in grade 2 and 3 encephalopathy survived, while 3 of 8 in grade4 expired. Mortality was similar in 2nd and 3rd trimesters. NANB virus was implicated in 62% deaths, hepatitis B in 25% and undefmed in 13%. A significantly higher rate of still birth was observed among the fatal cases.
Discussion
Acute viral hepatitis is the most common cause of jaundice in pregnant women6,7. Its frequency and severity is higherduringpregnancy in developing countries where higher incidences of fulminant hepatitis are seen. In this hospital based study of 53 pregnant women residing in the urban areas of Karachi city, the major identified cause of acute sporadic viral hepatitis was NANB virus (62%) and out of these cases, in 61% women the aetiology could be attributed to REV infection. Thus, of the total 53 cases, REVcouldbe implicated directly or indirectly in 21 cases (40%), makng it the most common cause of viral hepatitis in our pregnant women. Similar high rates have been reported in studies of acute sporadic viral hepatitis from other Afro-Asian countries, for example 81.6% from lndia8 and 59% from Ethiopia9. The low prevalence of hepatitis A in this study (4%) is in agreement with the previous seroprevalence studies revealing that 96-100% of our population is immune to this infection by the time they reach adulthood2. A 17% prevalence of acute hepatitis B is in agreement with reports from India8 while in strong contrast to a study from Kuwait which reported a fairly high incidence of acute hepatitis B (67%) among the pregnant women affected with viral hepatitis10. None of our patients were diagnosed as infected with hepatitis C virus. The antibodies to HCV usually becomes detectable 4-6 months after the onset of acute infection so even those 13 cases who were tested and were found seronegative at that time could, well be actually infected with this particular virus. Alternatively and more likely, it may be that none of our cases were due to acute viral hepatitis C, as this is an uncommon presentation of HCV infection. High maternal mortality is associated with fulniinant hepatitis during pregnancy in case of epidemics, but there are contradictory reports as far as sporadic fulniinant hepatitis is concerned. This study shows a high case fatality rate of 15% in acute viral hepatitis, 15% and 40% infulininant hepatic failure, which is in accordance with some recent studies of acute sporadic viral hepatitis having a case fatality rate ranging between 14-25%9,11,12.
Perinatal morbidity and mortality was very high, the most prevalent morbidity being pretenn delivery. Perinatal mortality rate was 30% which is in agreement with other studies reporting it between 20%-41%1,9,12,13. NANB virus was implicated as the etiological agent in majority of these reports. The cause of high maternal and fetal mortality particularly in those suffering from hepatitis NANB virus infection is not known. Investigators have suggested the possible role of nutritional and immunological factors14 but the subject has not been sufficiently studied. Malnutritionas a cause was ruled out in one of the studies in which 8 women who developed fulminant hepatitis were assessed as having excellent nutritional status15 . The other aspect possibly related to the increased severity may be an increased viral load.
Studies of pregnant women suffering from acute Lassa fever have shown an increased mean viral load in pregnant women compared to non-pregnant women16. The reasonforthis could be explained by the fmdmg of extremely high titer of virus in placental tissue suggesting thatthe placenta may beapmferred site forviral replication. Whetherany of the hepatitis viruses, particularly HEV, also preferentially replicate in placental tissue is not known. If this is proven it could explain the severity of viral hepatitis in pregnancy. The fact that the disease is severe if affects the women in 2nd or 3rd trimester could be because of the honnonal milieu at that stage of pregnancy favouring disease progression. Comparison of clinical and laboratory parameters of patients with fulminant hepatic failure with non-fulminant patients was done to identify poor prognostic factors. The significant factors were lack of antenatal care, increased severity of jaundice, history of somnolence, presence of gastro- intestinal bleeding at presentation and acute onset and rapid progression of illness.
This is in contrast to other observations in which survival is in fact increased lithe interval between the onset ofjaundice and the development of encephalopathy is less than 7 days17. In addition, to these serum bilirubin >10 mg/dl, abnormal prothmmbin time and raised BUN and creatinine were also identified as poor prognostic factors. When the same parameters were compared among fatal and non-fatal patients of FHF the only factor of prognostic significance identified was the grade of encephalopathy. The higher the grade, poorer the survival with a death rate of in patients with grade 4 encephalopathy. In summary enterically transmitted NANB virus seems to cause a high percentage of acute viral hepatitis in our obstetric population resulting in high case fatality rates.
The control of this enterically transmitted viral hepatitis remains a public challenge. Public health education programmes need to be undertaken to improve the awareness about this infection among the lay public. Virological surveillance of waste watercould help indeveloping strategies based onhygiene, sanitationand supply of safe drinkingwater.
Pregnant women affected with this illness should be provided institutionalised care and if any of the bad prognostic factors mentioned above are identified; intensive support therapy should be provided to improve the survival of these patients.
References
1. Sarkar, CS., Giri, AK. and Maity, T.K. Jaundice in pregnancy: Clinical study. J. Indian Med. Assoc., 1992;90:117-8.
2. Malik, LA., Legters, L.J, Luqman, M. et a!. The serological markers of hepatitis A and B in healthy population in northern Pakistan. J. Pak. Med. Assoc., 1988;38:69-72.
3. Qureshi, M.S., Ahmad, M., Rasbid, H eta!. Hepatitis Non.A, Non- B Report of water.borne outbreak. J. Pak. Med. Assoc., 1988;38:203-205.
4. Malik, IA., Luqman, M, Ahmad, A. et al. Sporadic Non-A, Non-B Hepatitis: A 6 sero-epidemiological study in urban population. J.Pak. Med. Assoc., 1987;37: 190.192.
5. Trey, C. and Davidson, L.S. The management offulininant hepatic failure. In: Popper, H., Schaffner, F. eds.Progress in liver disease. New York, Grune and Stratton, 1970, pp. 282-98.
6. Wilkinson, M.L. Diagnosis and management of liver disease in pregnancy. Adv. Intern. Med., 1990;35:289.310.
7. Ohazali, M., Morsad, F., Samouh, N. et at. Jaundice and pregnancy. The role of viral hepatitis. J. Gynecol. Obstet. Biot. Reprod. Paris, 1993;22:529-31.
8. Nayak, N.C.,Panda, S.K., Datta, R eta!. Actiology and outcome ofacuteviral hepatitis in pregnancy J. Gastroenterol. Hepatol., 1989;4:345-52.
9. Tsega, E., Hansson, B.G., Krawczynski, K. et al. Acute sporadic viral hepatitis in Ethiopia. Causes, risk factors and effects on pregnancy. Clin. Infect. Dis., 1992;14:96 1-965. -
10. Al.Kandari, S., Nordenfelt, E., Al-Nakib, B. etal. Viral hepatitis andpregnancy in Kuwait. Trans. R. Soc. Trop. Med. Hyg., 1987;81 :395-7.
11. Mirghani, O.A. Saeed, O.K. and Basama, F.M Viral hepatitis in pregnancy. East Air. Med. J., 1992;69:445-449.
12. De-Silva, H.J., Jayawardena, J., Pethiyagoda, AU. et at. Viral hepatitis complicating pregnancy . A five year hospital based retrospective study. Ceylon Med. 3., 1993;38:15-17.
13. Medhat, A., El-Sharkawy, MM, Shaaban, M.M eta!. Acute viral hepatitis in pregnancy. Int. J. GynaecoL Obstet., 1993;40:25.31.
14. O’Keefe, S.J.D., Carreker, T.E., El-Zayed, A.R. eta!. Malnutrition and immune incompetence in patients with liver disease. Lancet, 1980;2:615-617.
15. Khuroo, M.S., Tell, M.R., Skidmore, S. et al. Incidence and severity ofviral hepatitis in pregnancy. Am. J.Med., 1981 ;70:252-5.
16. Price, ME., Fisher H.S., Craven, RE. eta!. A prospective study of maternal and fetal outcome in acute Laasa fever infection during pregnancy. Br. Med. J., 1988;297:584-85.
17. O’Grady, 3G., Alexander, G.J.M., Hayllar, K.M. et at. Early indicators of prognosis in fulminant hepatic failure. Gastroenterology, 1989,97:439-445.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: