
Muhammad Umar ( Department of Surgery (Orthopaedics), The Aga Khan University, Karachi. )
August 1997, Volume 47, Issue 8
Original Article
Abstract
In an open prospective study the results of arthroscopic partial meniscectomy were reviewed in 188 knees. Group I comprised of 139 (65%) knees with pure meniscus lesions without any ligament laxity, the remaining 49 (35%) knees in group II had anterior cruciate ligament (ACL) deficiency in addition to meniscus lesions. Ingroup 1,93% had excellent to good and 7% had fair results by criteria of Tapper and Hoover1, In group II, 75% had excellent to good and 25% had fair results. Arthroscopic knee surgery was a good method of identifying patients in group II who required anterior cruciate reconstruction, One hundred (53%) sedentary workers were able to return to work at a mean time of 3 weeks. Patients classified as heavy labour comprised of a group of 40(21%) were able to return to their occupation in the mean time of 5 weeks. School and college students numbered 28 (14%) were able to go to their institutions in the mean time of 10 days. Twenty (9%) patients were professional or semi-professional athletes who were permitted sports training in 3 weeks and sports participation in 6 weeks on the average. There were no serious complications including wound infection, deep venous thrombosis (DVT) or loss of knee motion. The arthroscopic technique is reliable, cost effective and has high patient acceptance because of low morbidity and rapid return of good function to the knee joint (JPMA 47:210,1997).
Introduction
The first Arthroscopic Meniscectomy was peiformed by Masaki Watanabe2 in Japan in 1962 and was introduced in North America by O’Connor3 in 1977 including an operating arthroscope. Dandy4, Jackson5, Gillquist6 and Metcalf7 have been among the early pioneers ‘contributing to the development of arthmscopic surgical techniques, operating micro-instruments and power tools. The morbidity of arthroscopic meniscectomy of the knee is so low and return to normal function and sports activities so rapid that this technique has become very popular among the patients. Endoscopic surgery has virtually replaced open meniscus surgery wherever expertise in endoscopic surgery of the knee is available. Arthroscopic surgery of the knee was started at the Aga Khan University Hospital in April, 1990. Until December 1995, 221 such procedures have been done. The purpose of this study was to evaluate the effectiveness, safety, patient acceptance and economy of arthroscopic knee surgery in ambulatory settings in Karachi, Pakistan.
Patients and Methods
In an open prospective study, 221 patients underwent knee arthroscopy with a clinical diagnosis of torn meniscus, from April 1990 to December, 1995. The complaints in order of frequency were pain, inability to squat, giving way and recurrent knee swelling. The positive signs in order of frequency were joint line tenderness, obvious or subtle loss of terminal flexion or extension and joint effusion. One hundred and fifty (68%) patients had MRI of the knee confirming the diagnosis of torn meniscus while in the remaining 70 (32%), only the clinical diagnosis was relied upon. Internal derangement of the knee was a chronic problem (duration one year or more) in 180(90%) patients. Additional diagnosis of anterior cruciate ligament (ACL) deficiency was made in 31 knees clinically and in another 15 on MRI. These cases fell into two distinct groups. Group! consisting of pure meniscus lesions without any ligament laxity and group II with ACL deficiency in addition to memscus lesions. The arthroscopic surgery was carried out as an ambulatoiy procedure under general/spinal anaesthesiaexceptwbenpatients were from out of town necessitating overmight hospital stay in3O individuals.
Efforts were made to perfonn partial memscectomy and preserve a stable functional meniscus in all cases whenever possible.
Debridement of ACL stump was only done if it was felt to interfere with joint function. Incidental removal of cartilaginous/osteocartilaginous loose bodies were also carried out in 30 knees. Eight knees ingroup I with no unstable meniscus lesions on arthroscopy were excluded from the study, although, all these patients were reported to have complete tears of posterior third of medial meniscus onMRJ.
Four ACL deficiency knees in group II found to have no unstable meniscus lesion on arthroscopy were excluded from the study with recommendation of anterior cruciate reconstruction surgeiy. Patients were given long acting local anaesthetic (15 ml 0.5% Bupicain hydrochloride - 75 mg) intraarticularly at the end of the procedure and lower limb immobilized in a supportive dressing which provided very effective pain control for 12-24 hours post-operatively. Postoperatively patients were instructed in isometric quadriceps exercises and allowed partial weight beating on the lower limb as tolerated with awalldng aid. Patients were seen in the clinic on 3rd to 5th post-operative thy when dressings were removed and range of motion (ROM) and resistive muscle strengthening exercises were instituted. Further follow-up consisted of weekly check-ups for three weeks and then bi-weekly until the patient fully recovered, usually within S to 10 weeks. At the time of discharge, patients were encouraged forafollow-upvisitat3 months and one year post-operatively. Follow-up varied from a minimum of three months to a maximum of 4.5 years with a mean of 3.4 years in 90% of the patients in this study.
Results
One hundred ninety-three arthroscopic partial meniscectomies were performed in 188 knees. Five knees had simultaneous operations on torn medial and lateral menisci in ACL deficiency group. Group I with pure meniscus lesions without any ligament instability comprised of 139 patients with an age range of 14 to 50 years (mean 31 years) and male to female ratio of 10:1. Bucket handle and longitudinal tears were more common in younger patients with no orminüual degenerative changes in the joint. Cleavage and flap tears were prevalent in older patients with significant degenerative changes. Fifty-eight (40%) patients had sports related injuries, whereas, 65 (45%) patients had injured their knees during minor accidents and other activities of daily living and in 22 (15%) patients no definite injuries were reported.
Group II with ACL deficiency comprised of 49 knees (three knees added to the group based on arthroscopic fmdings) in 47, all male patients with an age range from 16 to 32 years (mean 25 years). Significant injury related to spoils activities or vehicular accidents was noted in all patients. Forty-two (80%) knees had significant degenerative changes in the medial/lateral orboth compartments. Medial to lateral meniscus lesion ratio was 3:1 inboth groups. Knees in group I and II were evaluated separately using Tapper and Hoover’s1 criteria of grading each knee as excellent, good, fair or poor. Excellent, a normal knee; good, the knee was functional in all activities including vigorous sports, but with some aching or swelling afterwards; fair, aknee giving definite symptoms and some disability, preventing vigorous sports; poor, a knee giving symptoms which interfered with routine daily activities.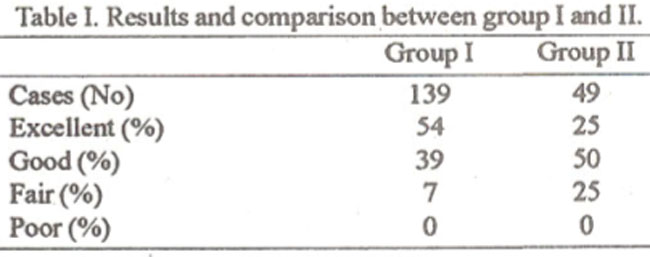
Table I shows functional grade and comparison between the two groups. Nine (7%) patients in group I in fair category, were mostly older patients with degenerative changes in the joint, who were symptomatic during sports activities such as squash, cricket and running. In Group II, all patients had unstable meniscus lesions in addition to ACL deficiency. Thirty-six (75%) patients benefitted from the procedure even though they had mild symptoms on demanding activities. Twelve (25%) patients in fair category continued to be symptomatic and were recommended to have anterior cmciate reconstruction surgery.
Occupational status:
One hundred (53%) patients were sedentary workers and were able to return to work at a mean time of 3 weeks. Forty (21%) patients involved in physically demanding industrial, agricultural or outdoor work, were able to return to their occupation in the mean time of 5 weeks. Twenty-eight (14%) patients were school or college students who were able to go to their institution in the mean time of 10 days. Threnty (9%) patients were professional or semi-professional athletes who were permitted sports training in three weeks and sports participation in 6 weeks on the average. No significant complications were noted in this series including infection, DVT or loss of knee motion. The results of this series are compared with open total meniscectomy series of Tapper and Hoover1 in Table II.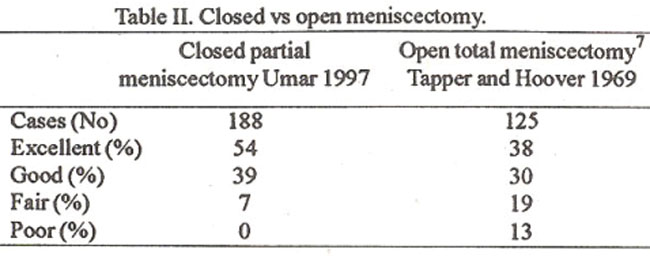
The results of endoscopic partial meniscectomy are superior to traditional open meniscectomy.
This is borne outby other endoscopics urgical seriesas well4,8. Azthmscopic partial meniscectomy results of the present series are compared with Northmore . Bail and Dandy8 (Table III).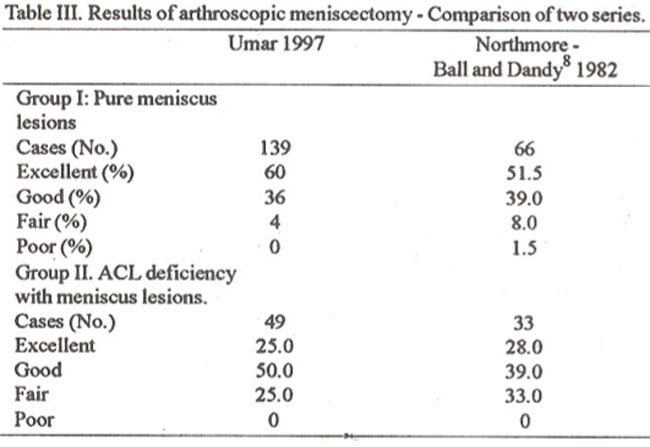
Discussion
One hundred and ninety three arthroscopic paitial meniscectomies were perfonned in 188 knees. Arthroscopic procedure was successful in 100% of the cases, thus avoiding the need for an open procedure. MRI is a highly sensitive test for picking high intensity signals in the memsci and intrameniscal degen9rative lesions especially in the posterior aspect of medial mehiscus may be diagnosed erroneously as full thickness tears9. Of 150 (68%) patients with a meniscus tear on MRl, 8(5%) were not found to have ameniscal tearon arthroscopy. Due to the presence of false positive tears, paitial meniscectomy should be restricted to those cases where unstable meniscus tear canbe demonstrated arthroscopically. MRI should be done whenthe cimcian is unceztain of both the diagnosis and need for arthmscopy. When a patient has clear cut history and typical fmdings of a torn meniscus, early arthroscopy will confirm the diagnosis and treat the condition in the same procedure9. In the current series 100 patients had MRI already done when first seen and in 80 of these, a certain clinical diagnosis of torn meniscus was possible. The over utilizations of this expensive study should be rationalized and reseived for cases of uncertain diagnosis only. The early and late results of traditional open meniscectomy have been extensively documented10-13. . The recovery of function is slow, residual loss of motion, persistent muscle atrophy and compromised function occurs in 15-20% of the patients.
Progressive degenerative changes in the knee are well documented on long term follow-up1,10,12 So impairment of function and disability on long tenn follow up is repoited 30% orhigher.
Tapper and Hoover1 and Cargill and Jackson12 suggested that partial memscectomy caused less degenerative changes than total meniscectomy in Bucket handle tears of meniscus. In 1954 Astrand13 reported better results by partial memscectomy as compared to open method. McGinty14 reported similarresults in 1977. However, limitingfactorwith open surgery was that technique called for displaced bucket handle tears only. Arthroscopic technique affords the opportunity to inspect and manipulate the entire meniscus and identify the fall extent of the lesion prior to excision. Artbroscopic technique and special instrumentation makes it possible to excise the lesion in any part of the meniscus. This selective meniscectomy aims at preserving a functioning meniscus. In this series, it was possible to accomplish the goal of selective (partial) meniscectomy in 160 (85%) knees. The remaining 28 (15%) knees required subtotal meniscectomy because of extensive and complex nature of memscal tears.
Arthroscopic partial meniscectomy is superior to traditional open meniscectomy because of the low morbidity, rapid rehabilitation, high patient acceptance and early returntowodc and sports. In the long run it is hoped that selective arthroscopic meniscectomy will minimize the degenerative changes inthe articular cartilage of the knee and report of long term results are encouraging8. Rockborn and Gilquist’5 have reported a 13 year physical and radiographic follow-up of 43 patients under 23 years of age. Atthe follow-up examinations, no differences in range of motion, muscle strengths or knee stability were seenbetweentheoperntedand the non-operated knees and 90% had no functional deterioration. However, 40%ofthe knees showed radiological progression (Fairbank’s changes) on the operated knees when compared to only 10% of the non-operated knees, but only 4% showed significant progression. In the present series, 80 patients with pure meniscus lesions were 30 years old or younger and only 45 had a mean follow-up of four years. Forty patients had bilateral pre-opemtive and recent post-operative knee x-rays available. Two (5%) knees showed degenerative changes and narrowing of medial joint space without deterioration of clinical ratings in these patients, however, duration of follow-up is only four years versus 10-13 years.
Covall and Wasilewski16 have reported radiologic changes after artbroscopic meniscectomy with five year follow-up in patients more than 45 years old. Sixty percent of post-operative knees showed radiologic progression of Fairbank’s changes compared with 20% of the non-opeiated knees. However, significant radiologic progression was noted in 15% in the operated knees and 11% ia the non-operated knees. In the present series patients above 45 years of age with a minimum follow-up offouryears was only 15. This number is too small for meaningful analysis, however, trend of degenerative changes is in keeping with the series noted above. It is quite clear that arthroscopic partial memscectomy does contribute to degenerative arthritis of the knee on along term follow-up, however impressive relief of symptoms, minimum morbidity and maintenance of good function for many years more than justifies arthmscopic meniscectomy. The endoscopic technique is ideally suited in Pakistani settings because invasive surgezy is associated with high rate of complications such as, infection and knee stiffness requiring prolonged treatment and physiotherapy especially because our medical facilities are not at par with international standards. There are significant cost savings because of elimination of hospitalization, intravenous antibiotics, quick recovezy and excellent prospects for full recovery and early return to work. As arthroscopic technique involves special dexterity and hand eye coordination, many orthopaedic surgeons may never become proficient in arthroscopy. Endoscopic meniscectomy is technically difficult to perform and requires special training. Sufficient experience in diagnostic arthroscopy is necessary before attempting endoscopic surgical meniscectomy. Gentle and atmumatic technique is required because it is easy to injure and damage the delicate articular cartilage with careless and clumsy use of instruments during endoscopic surgery. Because of low morbidity associated with the procedure, there is a risk of excessive use of this surgical modality. The use of arthroscopy should be restricted to well defined pathological conditions and should not replace gooa clinical judgement as medical technology is a good servant but a bad master.
References
1. Tapper, E.M and Hoover, N.W. Late results after meniscectomy. J. Bone Joint Surg., 1969;51 -A:5 17-20.
2. Watanabe, M, Takeda, S. and Ikeuchi, H. Atlas of Arthroscopy, ed. 2. Tokyo, Igaku shoin, 1969.
3. O’Connor, R.L. Arthroscopy. Philadelphia, J.B. Lippincott Co., 1977.
4. Dandy, D.J. Early results of closed partial meniscectomy. Br.Med.J., 1978;1:1099-1104.
5. Jackson, R.W. and Dandy, D.J. Arthroscopy of the knee, New York, Grune and Stratton Inc., 1976.
6. Gillquist, J. and Hagbeig, G. A new modification of the technique of arthroscopy of the knee joint Acts Chir. Scand., 1976;1 42:123-29.
7. Metcalf; R. Arthroscopic partial meniscectomy. Abstt Int. Soc. Knee, Lyon, 1st. Congress, 1979.
8. Northmore- Ball, MD. and Dandy, D.J. Long term results of arthroscopic partial meniscectomy. Clin. Orthop. 1982;167:34-39.
9. Peterfy,, C., Janzen, D. and Tirman, P. eta!. ‘Magic angle’ phenomenon: A case of increased signal inthenormal lateral meniscus on shortTE MR imagcsofthe knee. Ant J. Roentgenol, 1994;163:149-154.
10. Fairbanks, TJ. Knee changes after meniscectomy. J. Bone Joint Surg., 1948;30-B:664-67.
11. Smillie, 1.8. Injuries to the knee joint, ed. 5th., Edinburgh, Churchill Livingstone, 1978.
12. Cargill, OR. and Jackson, J.P. Bucket handle tear of the medial meniscus. J. Bone Joint Surg., 1976;58-A:248-53.
13. Astrand, T. Treatment ofmeniscus rupture ofthe kneejoint. Acts Chir. Scand., 1954; 107: 145-5 1.
14. McGinty, J.B., Geus, L.F. and Marvin, RA. Partial or total maniscectomy. J. Bone Joint Surg., 1977,59-A:763-66.
15. Rockbom, P. and Gillquist, J. Outcome of arthroscopic meniscectomy. A 13-year physical and radiologic follow-up of 43 patients under 23 years of age. Acts Orthop. Scandinavica, 1995 ;66:1 13-7.
16. Covall, D.J. and Wasilewski, S.A. Roeng enographic changes after arthroscopic meniscectomy: 5 year follow-up in patients more than 45 years old. Arthroscopy, 1992;8:242-6.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: