
Lubna A. Baig ( Faculty of Health Sciences, Baqai University, 51, Deh Tor Plaza, National Highway, Karachi. )
Inayat Thaver ( Faculty of Health Sciences, Baqai University, 51, Deh Tor Plaza, National Highway, Karachi. )
August 1997, Volume 47, Issue 8
Original Article
Abstract
The role of supervisors in diarrhoea case management at the Oral Rehydration Therapy (ORT) corners of Sindh was assessed by a random sample of 62 ORT corners in rural and urban areas of Sindh. The supervisors at each facility included, Medical Superintendents, District Health Officers, Senior Medical Officers, Civil Surgeons and Medical Officers. In 65% cases the supervisors were working at the same facility and in 35% the supervisors were based elsewhere. In 33.7% cases, there had been no meeting with the supervisor in the past 3 months which incidently was the diarrhoea season. In 6.5% cases there had been only 1 meeting, in &5% there had been 2-3 meetings and in the remaining 41.3% cases there had been more than 3 meetings with the supervisor. In majority of the cases the supervisors did not do anything related to improvement of diarrhoea case management. Supervisors had given some importance to case management in the urban areas and the Diarrhoea Training Units (DTU). The supervision at ORT facilities was found to be ala rudimentary level and it Is suspected that this might be adversely affecting the quality of diarrhoea case management (JPMA 47:208, 1997).
Introduction
Diarrhoea is still a killer of children under 5 years and according to a repoit by UNICEF every day 8,000 children die of diarrhoeal dehydration, a toll the world can and must reduce1. The morbidity of diarrhoea has not changed in the past 10 years. Prevalence in Pakistan is still at 42.8% and only 20.8% mothers are using ORS2. The incidence of diarrhoea in ahousehold survey conducted in Laikana was 5.1 episodesper child per year Diarrhoea is the main cause of malnutrition in Pakistan3 and a malnourished child grows as an unhealthy adult who may not be able to perfonn at an optimal level. In Paldstan, 40% of the under 5 children are underweight, with 14% severely malnourished4. The situation may be worse in the mm! areas, as only 35% of rural population has access to health services as compared to 99% of urban population. With a commitment to reduce diarrhoe al deaths, Pakistan formulated its National Policy on diarrhoea case management in 1988-89 5 and recommended the need for constant supervision of health workers at all facilities for controlling morbidity and mortality due to diarrhoea. The supervisors posted in the major health facilities, at district level were required to supervise the health workers in adjacent Basic Health Units (BHU) and Rural Health Centers (RHC). The supervisors were directed to meet the supervisees once aweek to once in a fortnight depending upon the distance of the BHIJ/RHC from the district health facility.
By the end of 1988, Pakistan had established 80 Diarrhoeal Training Units (DTUs), in collaboration with World Health Organization and 6973 Oral Rehydration Therapy (ORT) corners with the assistance of UNiCEF, Pakistan. The Diarrhoeal Disease Control (CDD) Programme of Pakistan conducted a survey in 48 health facilities in 1991 to assess the quality of case management of children with diarrhoea in healthfacilities and detectproblems in the facility supports (supervision, supplies) for appropriate case management6. This survey detected flaws in diarrhoea case management and recommended to improve supervision by providing guidelines for supervisors on diarrhoea case management The supervisors were instructed to guide the health workers for diarrhoea case management Afterall these efforts by the government and the related agencies a positive change was expected in the role of supervisors at the DTIJ’s and ORT corners with improvement in case management of diarrhoea This study was conducted to assess the role of supervisors in diarrhoea case management at the ORT corners of Sindh and to evaluate the effect of supervision on knowledge of health workers and quality of diarrhoea case management and supervision and lack of continued training/education of health care providers.
Subjects and Methods
This was a health systems research project adapted from the WHO health facility survey manual7. A total of 158 ORT corners and DTUs were identified in Sindh province. First urban and rural stratificationwas done “Districtwise” and then a systematic random sample of64 centers was drawn, through a WHO recommended health facility survey manual7 using sample size table for 95% precision. The sample included 38 rural ORT corners (only 36 were surveyed), 16 urban ORT corners and 10 Diarrhoea Training Units from all the 18 districts of Sindb. Three survey teams were formed and each team included 3 surveyors, with experience in health and college education and one supervisor, who was a doctor with experience in diarrhoea case management. Survey team was trained by the staff of diarrhoea training unit at Civil Hospital Karachi in diarrhoea case management and health facility survey technique. The questionnaires for assessing role of supervisors were modified from the WHO health facility survey manual. First, the health workers of ORT corners and DTU’s were observed for case management of diarrhoea and then interviewed for their knowledge and role of supervisor during last visit. All the records were checked for supervisors visits and comments of health workers after meeting the supervisor and were only taken for the previous 3 months to avoid recailbias. Variables included:
1. Role of supervisor:Observation of case management; Reviewing records and supplies.
2. Knowledge of Health worker: Case management of diarrhoea according to the ABC Plan3.
3. Case management of diarrhoea: Followng the ABC Planfor diarrhoea case management.
4. Records.
Results
A total of 62 centers were surveyed and 92 health workers were interviewed. Health workers included doctors and lady health visitors (LHV). Nurses present at the facility were notfound managing a diarrhoea patient, hence, they were not interviewed. The supervisors at each facility included: Medical Superintendents, District Health Officers, Senior Medical Officers, Civil Surgeons and Medical Officers. Of 92 health workers, 65% (n=60) had the supervisors working in the same facility, whereas 35%(n=32) health workers had the supervisors based elsewhere. Thirty-one (33.7%) health workers had had no meeting with their supervisors in the past 3 months which was the diarrhoea season. However,6 (6.5%) health workers said they had only 1 meeting, 17(18.5%) had 2-3 meetings and the remaining 38(41.3%) had more than 3 meetings with the supervisor. Regarding actual supervision condUcted by the supervisor, it was found that in majority of the cases the supervisors did not do any thing related to improvement of diarrhoea case management (Table I).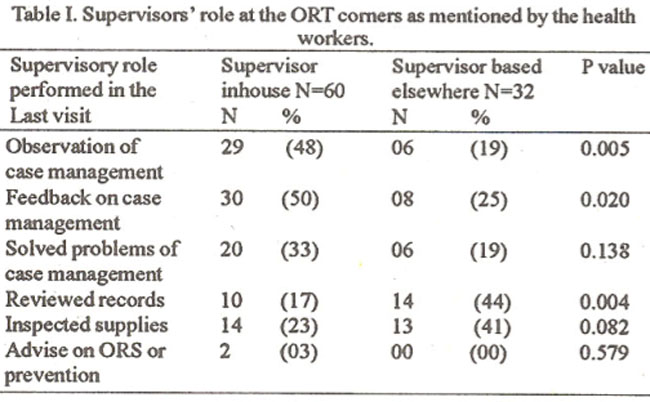
The supervisors gave importance to case management only in the urban ORT corners and DTU’s. Majority of the supervisors based at the same facility were observing case management (p<0.005) and giving feedback (p<0.020) to the health workers as compared to the supervisors based elsewhere (Table I). The supervisors coming for supervision from other facilities were reviewing records (p<0.004) more often than the inhouse supeivisors.The knowledge of health workers regarding history taking, examination and treatment of a diarrhoea! child was similar to those working with or without the supervisor in the same facility, .which means that the presence orabsenceof supervisors fmmthe facility showed no difference in the knowledge of health workers (Table II).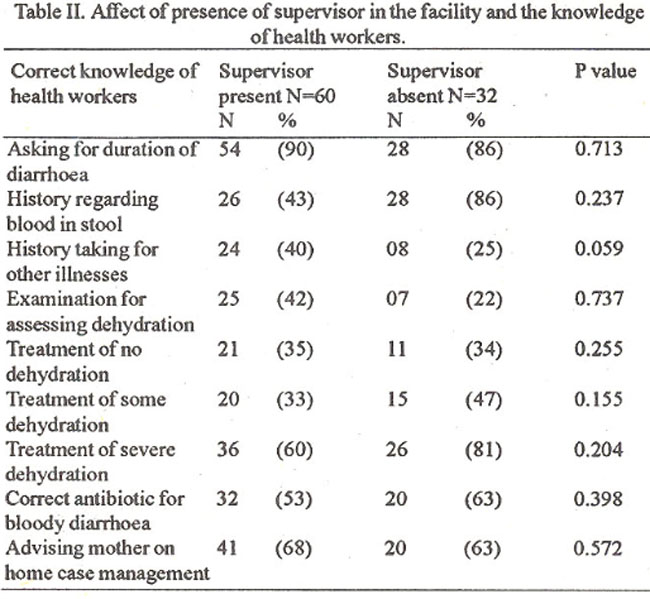
The same was observed in advice given to mothers for home care of a diarrhoeal child and diarrhoea case management (p<0.05).
Discussion
The supervisionforcase management and facilities was minimal. There was lack of supervised diarrhoea case management at all the facilities and the condition was worse at farfiung remote niral areas. There was not much difference in the findings of the present study and those reported in the previous studies5-7. The suggestions givenby previous studies included improvement in supervision at the ORT corners and training of the supervisors. We conducted this survey 4 years afterthese recommendations andfound no majorchange in the quality of supervision. Although presence and absence of supervisors was not affecting the knowledge or practice of health workers regarding diarrhoea case management, but their mere presence was felt as supportive by the health workers. Out of the 90 health workers who gave suggestions for improving quality of case management, 63 (68.5%) said that supervision during case management improves the quality of care. As the supervisors were not interviewed therefore, theirknowledge could notbe assessed. It is possible that they may not be trained themselves and henceforth avoided supervisionof diarrhoea case management. There is a need to qualitatively assess the role of supervisors and factors responsible for continued delay in strengthening of supervision at the ORT corners. There should be continuous on-the-job trainingof all health workers including supervisors for diarthoea case management. Supervisors should also be tiaincd in supervisory skills as medical/nursing graduates receive no formal training in skills of management. This concerted effort will then possibly improve quality of diarrhoea case management.
Acknowledgements
Authors acknowledge the support of Prof. M. Iliyas Dean, Faculty of Health Sciences, Baqai University, Dr. A.
Ghaffar Billoo Chairperson Department of Paediatrics, Dow Medical College, Dr. Capt. Mir Mohammed Sheikh, Project Director, Control of Diarrhoeal Diseases Pmgrainme. Sindh and Dr. AsifAslam Programme Officer, UNICEF, Sindh.
References
1. UNICEF. Thestate of world children. ORS: The medica! advance of the century. Ed. Grant, J.P., UNICEF, New York, Oxford University Press, 1996, pp. 58-59.
2. Khan,A. Child Hea!th National Hea!th Survey of Pakistan. lslamabad,Pakistan Medical Research Council prelixninaiy report, 1996. pp. 19.61.
3. Billoo, AG., Ahmed, S.T. and Habib, F. Epidemiology and etiology of diarrhoea. Management of diarrhoea in children. A manual for family physicians. Karachi Department of Paediatrics, Civil Hospital, 1995, pp. 06-12.
4. Synder, J.D. and Merson, M.H. The magnitude of the global problem of acute diarrhoeal disease: A review of active surveillance data. Bull. WHO., 1982;60:605-6 13.
5. UNICEF. The state of the world children. Ed. Grant, J.P. UNICEF, New York, Oxford University Press, 1996, p. 84.
6. World Health Organization. Programme for control of diarrhoeal diseases: SeventhProgrammerepozt 1988-1989: Geneva, WHO/CDD/90.34.
7. Health Facility Survey of Diarrhoea Case Management: Ministry of Health, Diarrhoea! Disease Control Programme of Pakistan and Programme for the Control of Diarrhoea! Diseases. Geneva, World Health Organization. Geneva, 1991.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: