
Farida Agha ( PMRC Central Research Centre, Islamabad. )
Agha Sadaruddin ( PMRC Central Research Centre, Islamabad. )
Shahid Abbas ( Department of Allergy and lmmunology, National Institute of Health, Islamabad. )
S. Mohsin Ali ( PMRC Central Research Centre, Islamabad. )
June 1997, Volume 47, Issue 6
Original Article
Abstract
Total serum IgE levels were estimated in 219 patients with various allergic disorders (119 with bronchial asthma, 68 with allergic rhinitis and 32 with urticaria) and 240 healthy age matched subjects. Serum IgE levels were significantly (P<0.001)higher in healthy males (mean 181 IU/ml) than females (mean 99 IU/ml).
Higher levels were found in the age group 15 to 24 years and lowest in over 55 years. Males had higher I8E levels than females at any given age. Mean IgE levels were significantly (p<0.001) higher in all three groups of patients than in healthy subjects. Among all age groups, the difference In mean IgE levels between allergic subjects and controls was significant. Positive skin test reactivity (to pollen and dust allergens) was found in 60% patients with asthma, 51% with allergic rhinitis, 46% with urticaria and in 4.5% healthy subjects. Patients with positive skin test had higher mean IgE levels as compared to those with negative skin test, but the difference was insignificant (JPMA 47: 166,1997).
Introduction
Immunoglobulin E (IgE) holds a unique position among immunoglobulins. It is normally present in human serum in extremely small amounts, its serum concentration may increase several hundred fold in response to specific stimuli1,2. Since its ‘discoveiy3,4, IgE has been studied in various patients5-8 and population studies. The immunologic response of individuals exposed to similarenviromnents is not uniform and a wide range of serum IgE levels has been reported in unselected adults4-9. The levels are increased in allergic diseases like allergic rhinitis, allergic bronchial asthma and atopic dermatitis or urticaria9-15. The present study was undertaken to estimate the serum total IgE levels in patients with various allergic disorders and compare them with those, found in healthy subjects of similar age groups. Correlations of serum IgE with age, sex and skin test reactivity was also detemiined.
Patients and Methods
A total of 219 patients with various allergic problems, attending the Allergy Centre in Clinical Research Division (CRD), National Institute of Health (NIH), Islamabad, were included. Age, sex, socioeconomic status, family history of allergy, history of receiving drug therapy both prior to and duringthe study were recorded. Eachpatientwas examinedby the physician and diagnosis for allergy was established by using information given by patient, as well as by consulting the result of the physical examination and skin test. The diagnosis cnteria for asthma included a perenial or seasonal history of wheezing and shortness of breath which resolved either spontaneously or on treatment with bronchodilators, Allergic rhinitis was defined as sneezing, rhinorrhoea and nasal obstruction. Urticaria was diagnosed by localized vasodilation (ezythema), transudation of fluid (wheal) and flaring due to local axon reflex, A total of 240 healthy age matched subjects who had no history of allergy were selected as controls.
Allergen skin test
Drops of battery of allergens10-15 were placed on the volar surface of the arm and pricked with the standard disposable lancet. The drops were then mopped up by tissue paper and patient was asked to wait for 10-15 minutes. The arm was then examined for the presence of wheal and flare. The average diameter of more than 2 mm was taken as positive. Skin prick test was performed in all patients and controls using common allergens mixed pollens (paper mulberry, dandlion) and dust (house dust). In some patients mixed protein allergen (beef, mutton, fish, egg, chicken, wheat) were also used in addition to pollen and dust.
IgE determinations
Blood samples for IgE determination were obtained prior to any immunotherapy. Total serum IgE was detennined by Immunoenzymetric Assay (Coated tube) using the total IgE Serozyme kit from serono diagnostics. The method can be used for samples over the range zero to 800 IU/ml without dilution. Standards were calibrated against the WHO, 2nd International Reference preparation (JRP) for human serum IgE.
Statistical analysis
Serum IgE levels were converted to logio for calculations because the frequency distribution of IgE levels were skewed and were unsuitable for application of analysis assuming normal distribution of variables16. The transformation converted the data into suitable form. All analysis on IgE were therefore carried out on transformed data and anti-log or geometric mean values were also used for display in tables and for comparison. The students test was used to test for differences between groups.
Results
Two hundred and forty healthy subjects (156 males, 84 females) and 219 patients suffering from allergic disorders which included 119 patients with bronchial asthma (58 males, 61 females), 68 with allergic rhinitis (38 males, 30 females) and 32 with urticaria(18 males, 14 females) were studied. The mean age of patients and controls is shown in Table I.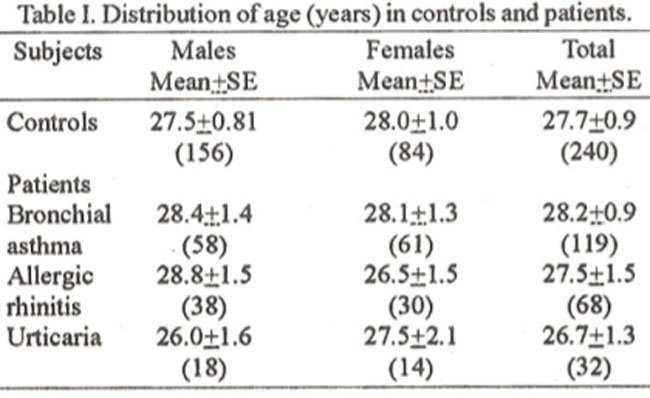
The distributionof IgE levels with relationto age and sàxinhealthy subjects is shown in figure. Priorto logarithmic conversion, the distribution was skewed, with almost 30% of the values over 200 lU/mi and 12% as high as 800 lU/mi, At the other extreme the lowest recorded value 10 lU/mi was found in 1.25% subjects and 7% of the subjects had values between 20 and 40 lU/mi. Following logarithmic conversion, the distribution of values becomes normal with mean logio IgE 2.17 lU/mi and a geometric mean of 148 lU/ml. A significant sex difference (P<0.001) in mean IgE levels was found in healthy subjects. Males had significantly higher mean IgE levels (181 IU/ml) than females (99 lU/mi). Highest levels were found in males among 15 to 24 years old and in females among 25-34 years old (Figure). Levels in males over 55 years (64 lU/mi) were significantly lower than in young adult males (216 lU/mi). In all age groups the mean IgE levels were significantly higher in males than in females except for the group 45 to 54 years where the difference was statistically insignificant (Figure).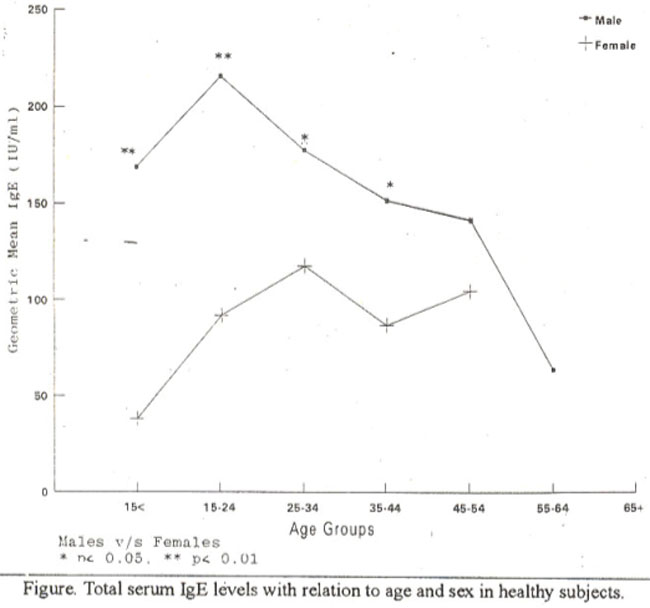
In allergic subjects no significant difference was found in mean lgE levels between the two sexes and age. Mean Semm IgE levels (1U/ml) indifferentgroups of allergic subjects and controls is shown in Table II.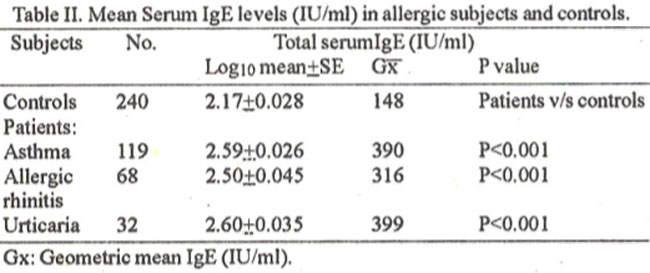
Levels were more than twice as high in allergic subjects than in controls. The difference was highly significant (P<0.001) in all three groups of patients as compared to controls. However, no significant difference was found in mean IgE levels between the different groups of patients. Comparison of mean IgE levels (lU/mI) at various age groups in allergic subjects with controls is shown in Table III.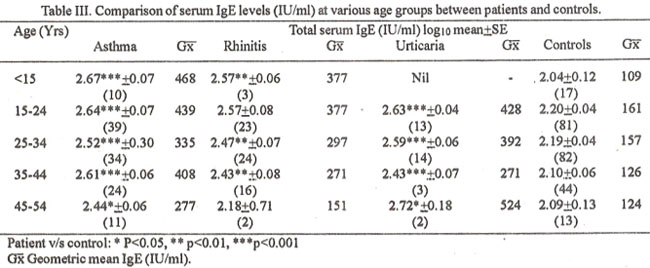
The mean levels were significantly higher among all age groups in allergic subjects as compared to controls. The difference was more significant at younger age (15-24 years) than at 45 years and above. Allergen skin test reactivity in allergic subjects and mean serum IgE levels (lU/mi) is shown in Table IV.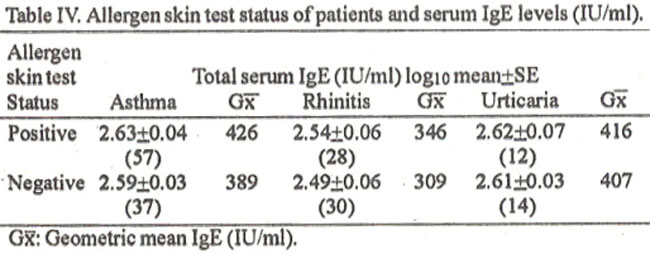
The skin prick test (for both pollen and dust allergens) was positive in 60% patients with asthma, 51% with allergic rhinitis and 46% with urticaria. Only 4.5% (11/240) healthy subjects showed positive skin test. Fourpatients with urticaria showed positive skin test to mixed protein. The mean IgE levels were higher in patients with positive skin test as compared to those with negative skin tests, however the difference was statistically insigimficant (Table IV).
Discussion
A wide variation in serum IgE levels has been documented in various Several authors have attempted to define nonnal levels and ranges in healthy non-allergic adult populations19-21. Because of the widerange of serum IgE levels it has been extremely difficult to establish reliable ranges or 95% confidence limits for this immunoglobulin19. The variation in values are probably related to a different technique used for measuring IgE, to different populations studied and possibly to the use of a different standard7. In addition to variations in experimental results, there also is a problem in appropriately expressing mean values for normal subjects or various groups of patients19. The skewed distribution of IgE in all populations that have been studied has made it necessaiy to convert from arithmetic to logarithmic values in reporting group means and ranges7,10,12,14,16,18,19,22. Similarly in the present study a normal distribution occurs following logarithmic conversion, witha geometric meanvalue of 148 lU/mi forhealthy subjects.
Bathee et al19 reported a geometric mean value of 32.1 lU/ml in 2743 subjects (aged 6 to 90 years), with and without evidence of atopy. They found 12.1% of values greater than 200 lU/mi and 40% below 20 lU/ml.. We found 30% of the values above 200 lU/mi and 1.6% were below 20 lU/mi. In another study16 the geometric mean was 320 lU/mi in 97 non-allergic black individuals and 123 lU/mI in 53 non-allergic white individuals. Grove et al22 reported a geometric mean value of 98 lU/mi in 100 control subjects. A study from Pakistan23 reported a normal mean value of 75.3 IU/ml for 200 healthy subjects using radial immunodiffusion technique. Aside from technological and methodological differences, the variation in values may also depend on the extent to which the study population was random or selectively non-atopic. Age and sex relationship also exists with regard to IgE for healthy subjects19,20. The peak levels +Femle are reached during the latter half of the first and be inning of the second decade, then declines thereafter reaching a low level in subjects overage 75 years19. Males have higher levels than females at any given age19. Our data is in agreement with the above resorted findings. Similarly as reported by other workers7,16,23 we also found no significant difference in IgE levels between males and females in overall and at various age groups within all three groups of patients. The significant elevation of IgE levels in allergic subjects found in present study has also been reported by others5,7,8,11,16,19,23-26. The geometric mean values for asthmatics were about twice as high as in non-allergic individuals16. The levels were much higher in asthma than in rhinitis11,16. Similarfindings are seen in this study. However, we found elevated IgE levels in patients with urticaria as compared to others7,11,17. Aside from food allergy as some of these patients have shown by positive skin test, the possibility of parasitic infestation may not be excluded19,24.
Widely variable skin test reaction rates have been reported among various population groups27,28, depending upon the number and type of allergens used, the skin test method employed and the extent to which allergic subjects have been included or excluded. The prevalence rate in non-allergic individuals varied from 9 to 50%27,30. We found a 4.5% reactivity in our carefully selected normal subjects. A study from Pakistan31 reported prevalence of skin allergy test, using ten common allergens among 23 patients with chronic obstructive pulmonary disease, the test was positive in 56% patients who were active smokers, in 14% ex-smokers and in 30% controls. The atopic group of patients with positive skin test that correlated with their persoal history had significantly higher mean IgE levels than the non-atopic and normal subjects5,7,8,10,11,17,19,24-27. In present study though the values were higher in patients who had positive skin reactions than those with negative skin test but the difference was not statistically significant. However, patients who had elevated IgE levels but with negative skin test had history of allergy to a wide variety of allergens including histories of food allergy. Some patients also had family history of atopic disease. As most of our patients were skin tested with pollen and dust allergens and food allergens were used only in a few cases, it appears that there may be some other allergenic factors or conditions that may elevate IgE levels. Further we did not test for parasites and therefore cannot exclude the possible effects of parasitic infestation on IgE levels19,24.
This study highlights the need fora more detailed study to measure the year round concentrations of multiple aem-allergens found in our environment, to assess the actual prevalence of allergen skin test reactivity, its relationship with serum IgE concentration and the development of allergic and/or respiratory symptoms.
Acknowledgement
We are thankful to Mr. Sheikh Salahuddin, Superintendent, PMRC Central Reseaivh Centre, N.I.H., Islamabad for typing this manuscript.
References
1. Ishizaka, K., Ishizaka, T and Hornbrook, M.M. Allergen Binding activity ofE. G and A antibodies in sera from atopic patients; In-vitro-measurements of reaginic antibody. J. Immunol., 1967;98:490-492
2. Wide, L., Bennich, H. and Johansson, S.G.O. Diagnosis ofallergy by an in-vitro test for allergen antibodies. Lancet, 1967;2:1105- 1107.
3. Ishizaka, K. and Ishizaka, T. Identification of y E. antibodies as a carrier of reagmic activity. 3. Immunol., 1967;99: 1187-89.
4. Johansson, S,G.O, Bennich, H. and Wide, L. A new class of immunoglobulins in human serum. Immunology, 1968;14:265-68.
5. Johansson, S.G.O., Raised levels of a new immunoglobulin class (IgND) in asthma. Lancet, 1967;11:951-953.
6. Gleich, G,J., Averbeck, A. J. and Swedlund, HA. Measurement of IgE innormal and allergic serum byradioimmunoassay. 3. Lab. Clin. Med., 1971;77:690-692.
7. Spitz, E., Gelfard, E.W., Sleffer, AL. et al. Serum IgE in clinical immunology and allergy. 3. Allergy Clin. Immunol, 1972;49:337.47.
8. Leoffler, J.A., Cawley, L.P. and Moeder, M. Serum IgE levels: Correlations with skin test sensitivity. Ann. Allergy, 1973 ;3 1:331-36.
9. Johansson, S.G.O. Serum ND levels in healthy children and adults. Int. Arch. Allergy Appl. Immunol., 1968;34: 1-3.
10. Bazaral, M., Orgel, A. and Hamberger, R.A. Genetic of IgE and allergy: Serum IgE levels in twins. 3. Allergy Clin. Immunol., 1974;54:288-304.
11. Handerson, L.L., Swedlung, H.A., Van Dellen, R.G. et al, Evaluation ofigE tests in allergy practice. 3. Allergy Clin. Immunol., 1971;48:305-1 2.
12. Kumar, L., Newcomb, R.W. and Hombrook, M.A. A year round study of serum IgE levels in asthmatic children. J. Allergy Clin. Immunol., 1971;48:305-312.
13. Hoffman, DR., Yamamoto, F.Y., Geller, V. et al. Specific IgE antibodies in atopic eczema, J. Allergy Clin. Immunol., 1975;55:256-267.
14. McGeady, S.J. and Buckley, R.H. Depression of cell mediated immunity in atopic eczema. 3. Allergy Clin. Immunol., 1975;56:393-406.
15. Orgel, HA., Hamberger, R.H., Bazaral, M. et al. Development of IgE and allergy in infancy. 3. Allergy Clin. Immunol., 1975;56:296-307.
16. Grundbacher, F.J. and Massie, F.S. Level of immunoglobulin G. M.A. and Eat various ages in allergic and non allergic black and white individuals. J. Allergy Chin. Immunol., 1985;75:651-58.
17. Arbesman, C.E., Ito, K., Wypych, 3.1. et al. Measurement of serum lgE by a one-step single radial radiodiffusion method. J. Allergy Clin. lmmunol., 1972;49:72-80.
18. Orgel, HA., Lenoir, MA. and Bazaral, M. Serum IgG, IgA, IgM and IgE levels and allergy in Filipino children in the United States. 3. Allergy Clin. Immunol., 1974;53:2 13-222.
19. Barbee, R.A., Halonen,M., Lebowitz, M. et al. Distribution of lgE incommunity population sample: Correlations with age, sex and allergen skin test reactivity. 3. Allergy Clin. Immunol,, 1981;68:106-111.
20. Rowe, D.S. and Wood, C.B.S. The measurement of serum IgE levels in healthy adults and children and in children with allergic asthma. Int. Arch. Allergy, 1970;39:1-4.
21. Nye, L., Merrett, TG., London, 3. et al. A detailed investigation of circulating IgE levels in a normal population. Clin. Allergy, 1975; 1:13-16.
22. Grove, DI., Burston, TO.. Wellby, M.L. et al. Humoral and cellular immunity in asthma. 3. Allergy Clin. Immunol., 1975;55:151-163.
23. Saeed, S. and Siddiqui, S,A. A comparative study of serum immunoglobulin E levels in patients with allergic disease and healthy subjects. Pak. J. Med. Res., 1994;33:255-257.
24. Larrick, J.W., Buckley, C.E., Machamer, C.E. et al. Does hyperimmunoglobuIinemia-E protect tropical populations from allergic disease? 3. Allergy Clin. Immunol.. 1983,71:184-188.
25. Burrows, B., Halomen, M., Lebowitz, M.D. et al. The relationship of serum immunoglobulin E allergy skin tests and smoking to respiratory disorders. J. Allergy Clin. Imrnunol., 1982;70: 199- 204.
26. Dave, N.K., Hopp, R.J., Biven, RE. et al. Persistence of increased non-specific bronchial reactivity in allergic children and adolescents. J. Allergy Clin. Immunol., 1990;86:147-53.
27. Barbee, RA., Brown, W.G., Kaltenbom, W. et al. Allergen skin test reactivity in a community population sample: Correlation with age, histamin skin reactions and total serum Immunoglobulin E. J. Allergy Clin. Immunol., 1981 ;68:l5-19.
28. Barbee, R.A., Kaltenborn, W., Lebowitz, M.D. et al. Longitudinal changes in allergen skin test reactivity in community population sample. J. Allergy Clin. Immunol., 1987;79: 16-24.
29. Haahtela, T.,Bjorksten, F., Heiskala, M. et at. Skin prick test reactivity to common allergens in Finnish adolescents. Allergy, 1980;35:425-31.
30. Mensinga, T.T., Scghouten, J.P., Rijcken, B. et al. The relationship of eosinophilia and positive skin test reactivity to respiratory symptom prevalence in a community based population study. 3. Allergy Clin. Immunol., 1990;86:99-107.
31. Bokhsri, S.N.H. Markers of allergy among patients with chronic obstructive pulmonary disease. Pak. 3. Med. Res., 1990;29:20-22.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: