
O.N. Onwuanyi ( Department of Surgery, University of Benin Teaching Hospital, PMB 1111, Benin City, Nigeria. )
K.A. Omotosho ( Department of Surgery, University of Benin Teaching Hospital, PMB 1111, Benin City, Nigeria. )
K.A. Habeeb ( Department of Surgery, University of Benin Teaching Hospital, PMB 1111, Benin City, Nigeria. )
June 1997, Volume 47, Issue 6
Original Article
Abstract
A preliminary study of 15 patients undergoing extraction of Kuntscher nails after fracture surgery under local anaesthesia indicated varying behavioural responses and tolerance of the procedure. In the main study cohort, of 59 (fifty-nine) patients within the age range of 16-65 years, made up of 41 males and 18 females, 38 patients (64.4%) tolerated the procedure without discomfort, 14 patients (23.7%) experienced mild to moderate pain, while the remaining 7 patients (11.9%), pain and discomfort was severe enough to require the additional use of intravenous anaesthesia (Ketamine Hydrochloride). There were no significant complications post-operatively. Financial considerations are assuming a greater importance, since planned procedures for osteosynthetic metal implants removal contribute considerably to the waiting lists for elective surgery. We conclude that there are clear ad vantages in removal of Kuntscher nails under local anaesthesia and it is also noteworthy that the compliance rate amongst our patients has been on the increase, as this method offers shorter waiting period, immediate ambulation, is a day procedure, early return to work and lower monetary costs. We are unaware of existing prospective work on the extraction of Kuntscher nails under local anaesthesia (JPMA 47:153, 1997).
Introduction
Local anaesthesia has been extensively used in other surgical procedures such as herniorrhaphy1-3 and its advantages include: immediate postoperative ambulation, imposition of a gentle technique on the surgeon, avoidance of-post-anaesthetic complications, reduction in costs and waiting lists for elective surgery4-5. In developing countries the place of local anaesthesia becomes very relevant because of the shortage of qualified personnel and the inadequate supply of anaesthetic gases and equipment. Internal fixation in the management of fractures has been used with increasing frequency in recent years and operations for removal of metal implants have likewise increased. These procedures now account for 11% of all elective orthopaedic surgical procedures6. There have been controversies surrounding routine implant removal, with some authorities supporting this, because of osteopenia, fatigue fracture, metal corrosion and the rare occurrence of tumours in association with implants in both animals and man7,8. Also operations for the removal of implants have attendant risks and substantial have been reported9-11. As financial constraints increase and waiting lists lengthen, the need for removal of implants under local anaesthesia become important. What is more, as already indicated, this situation becomes more critical in a developing countiy with dire limitations in material and human resources.
We also note that many patients who have had Kuntschernail implants forfemoral fracture holdanerroneous view that surgery for its removal involves re-opening the fracture wound with further hospital stay and as such fail to respond positively. Extraction under local anaesthesia, immediate post-operative ambulation and subsequent discharge onthe same day has developed afresh enthusiasm in hitherto sceptic patients, This certainly means reduction in financial costs, immediate or early return to work and business. We present a cohort of 74 patients who were studied prospectively for tolerance to the removal of four Kuntscher femoral implant under local anaesthesia.
Patients and Methods
This consisted of a preliminary and main studies involving 15 and 59 patients respectively. This was undertaken through September, 1989 to October, 1993. Only patients with middle-third transverse or short oblique fractures were considered. Kuntscher nails (clover -leaf) were inserted without preliminaiy reamoring of the medullary canal. This we believe, protects the endosteal blood supply and similar view is shared by other workers12-14. The size of implant inserted ranged from 8/32 to 11/42 and was determined by trial with several sizes until a well-fitting nail was selected. All patients had a premedication of 75- 100 mg of intramuscular pethidine (according to body weight) and 10 mg diazepam 30 mins. before operation. No children under 16 years of age were included in the study.
Exclusion criteria were nail tip covered by bone (myositis ossificans), nail tip which is not projecting beyond piriforms fossa by about 2 cm. and a large K-nail which does not show on x-rays. Signs of loosening at the time of removal.
Local anaesthesia was achieved with the infiltration of plain Xylocaine of volume between 15-20 mIs of 1% solution around the incisional scar through which the implant was inserted in the gluteal area. All the patients had a single dose of intravenous ceftazidine pentahydrate (Fortum-Glaxo) 1.0 gm at the start of the procedure. All stitches were removed after two weeks during routine out-patient clinic visit. After the procedure, the patients were allowed to rest in the day ward for 4 hours and then went home the same day.
Informed consent for all the participants was obtained and 100% of those approached gave consent. Five surgeons performed the procedure on atleast 10 patients each. At the start of the operation, the patient was instructed to speak out if he/she felt discomfort or pain and throughout the procedure, two independent observers at the head of the operating table recorded the patients reaction, change infacial expression and movements. Kuntscher nails were removed with a nail extractor, the wound closed in two layers with chromic catgut and interrupted nylon sutures for skin. The type of femoral fracture, size of Kuntscher nail, period of implantation, the indication for removal, tolerance to the procedure and complication after surgery were noted. All nails were extracted within the period of 11-14 months of implantation. These patients were admitted under the care of one of three consultant orthopaedic surgeons. There were no patients under sixteen years of age.
Results
Thirty-eight (64.4%) patients felt no pain or discomfort and slept throughout the procedure, 14 patients (23.7%) experienced mild to moderate discomfort and in the last 7 patients (11.9%) the degree of pain was severe enough to warrant the additional use of intravenous ketamine in order to complete the procedure. Thirty of the patients who felt no discomfort, thirteen (13) of the fourteen (14) with mild to moderate discomfort and four (4) out of the seven (7) with severe discomfort preferred the use of local anaesthesia, for reasons, related to operational costs, immediate ambulation, short hospital stay and early return to work or business Table III).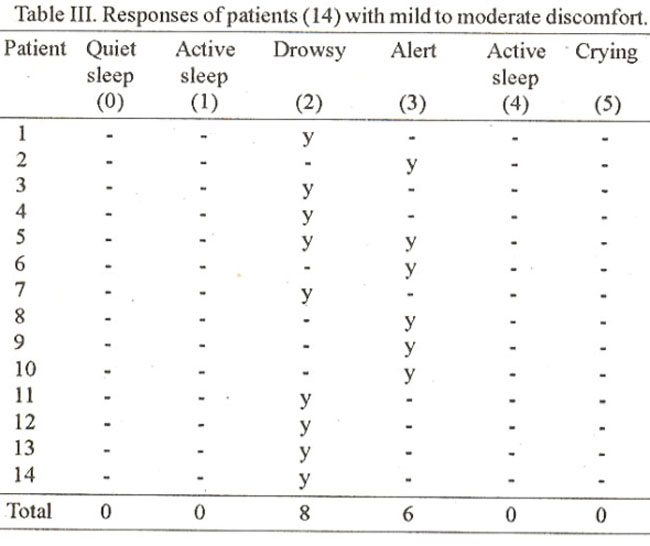
The average period of operation was between 30- 45 minutes. Fourpatients had woundinfection(3 with superficial dehiscence and the fourth had wound abscess).
Acknowledgements
We are grateful to Dr.Omotosho, Umebese and Onwuanyi for the inclusion of their patients in this study. Our thanks also go to the Surgeons who operated on the cases and Mr. Godday Aigbomian for secretarial help.
Discussion
For an effective assessment of patients’ tolerance of the extraction of Kuntscher nails under local anaesthesia, one must deliberately question the patient during the procedure and this could then be expressed in a scoring system as indicated on Table I.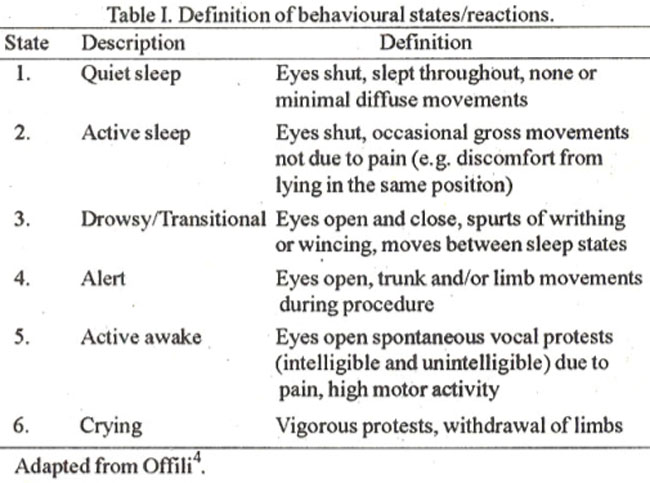
Thus, apart fmm variation in countenance, movement and spontaneous vocal protests of discomfort which some patients may bear stoically and thus fail to register these, no further criteria has been employed in this study. The value of using drugs with sedative properties as premedication in order to achieve better per-operative cooperation in patients undergoing minor surgery under local anaesthesia is well established2,3. That a significant population in the study group had no discomfort or mild discomfort and preferred local anaesthesia would suggest satisfactory tolerance of the procedure (Table II).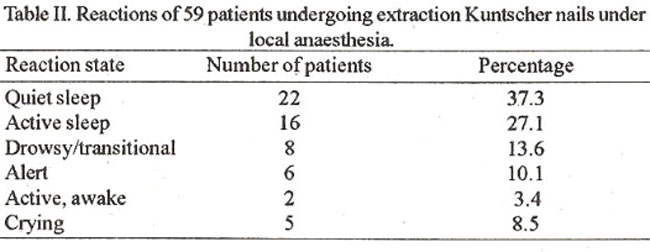
Pethidine with its dual effect as a sedative and centrally active analgesic would have contributed to the incidence of patients in this group. Further value of local anaesthesia for the removal of K-nails can found in its being a day case procedure, immediate ambulation and return to work with which most of the patients showed acceptance. It is noteworthy that four patients in the group with severe discomfort preferred local, anaesthesia but the procedure had to be completed with Ketamine fortechnical reasons, which meant greater deal of manipulation. In this situation, a female aged 26 years, the procedure was modified due to fear and apprehension and lastly in the fourth a male aged 50 years, the nail had migrated caudally leaving its upper end buried in the fossa piriformis of the femur. It is thus recommended that the nails be left high (about 2cm) above the pinforms fossato aid their removal. The average financial cost to the patient was N350.00 (Three hundred and fifty Naira) as against N1,500.00 (One thousand and five hundred Naira) for the same elective procedure under general anaesthesia exclusive of bed fees. This is statistically significant. There were no serious complications such as reaction to use of Xylocaine, refracture, persistent pain, recorded in this study (P>0.0 1). We should conclude that the benefits from the use of local anaesthesia for the extraction of femoral nail (Kuntscher) outweigh the risks. It is also necessary to support the views of other authors12-15 that implant removal may be technically demanding and should not be left in the hands of the inexperienced Surgeons. We are also unaware of a similar prospective work on implant extraction under local anaesthesia.
References
1. Ruckely, C,.V. Day care and short stay surgery for hernia. Review article. Br.J. Surg., 1978;65:1-4.
2. Glassow, F. Inguinal hernia repair using local anaesthesia. Ann. R. Coil. Surg. EngI., 1984;66:382-387.
3. Nicholls, J.C. Necessity into choice. An appraisal of inguinal hemiorrhaphy under local anaesthesia. Ann. R. Coil. Surg. Engi., 1977;59: 124-127.
4. Ofili, 0.0., Osime, U. and Morgan, A.A. Local anaesthesia in inguinal hernia repair: A system ofobjective assessment ofpatients’ tolerance. J. R. Coil. Edin., 1988,33:71-74.
5. Far-Guaharson, EL. Early ambulation with special reference to hemiorrhaphy as an out-patient procedure. Lancet, 1955;Il:5 17- 519.
6. Brown; R.M., Wright, E.F. and Chaimers, J. Removal of implants after fracture surgery - indications and complications. J.R. Coil. Edin., 1993;38:96- 100.
7. Sinbaldi, K.. Rosen, H., Luis, S.K. et al. Tumors associated with metallic implants in animals. Clin. Orthop., 1976;118:257-266.
8. Hughes, A.W., Sherlock, D.A., Hamblen, D.L. et al. Sarcoma at the site of a single Hip screw: A case report. J. Bone Joint Surg., (Br.) 1987;69B:470-472.
9. Raahave, D. Post-operative wound infection after implant and removal of osteosynthetic material. Acta Orthop., 1976;47:28-35.
10. Deluca. P.A.,Lindsey. R.W. and Ruwe, PA. Refracture of bones of the forearm after removal of compression plates. J. Bone Joint Surg. (AM.), 1988,70A: 13,72-76.
11. Perren, SM., Cordey, J., Gautier. E. et al. Early temporary porosis of bone induced by internal fixation implants. Clin. Orthop.. 1988,232:139-151.
12. Rowley, D.I. (Editorial) Removal of unnecessary implants. J. R. Coil. Surg. (Edin.), 1991;36:5.
13. Melcher, G. A., Rye, C.H. ,Leutenegger, A. et al. Tibia! fractures treated with the A 0 unreamed tibial nail. Injury, 1993;24:407- 410.
14. Klein, M.P.M., Rahn. BA. and Frigg, R. Reaming versus non- reaming in medullary nailing interference with cortical circulation of the caninetibia. Arch. Orthop. Trauma Surg., 1990;109:314.
15. Rush, J. The kuntscher rod in the treatment of femoral shaft fractures. Aust. N.Z.J. Surg., 1970;40:44.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: