
Tahir Jameel ( Department of Haematology and Genetics, Armed Forces Institute of Pathology, Rawalpindi. )
Yasmin Rashid ( Department of Haematology and Genetics, Armed Forces Institute of Pathology, Rawalpindi. )
Masood Anwar ( Department of Haematology and Genetics, Armed Forces Institute of Pathology, Rawalpindi. )
Nadira Sultana ( Department of Haematology and Genetics, Armed Forces Institute of Pathology, Rawalpindi. )
Muhammad Amin Waqar ( Department of Haematology and Genetics, Armed Forces Institute of Pathology, Rawalpindi. )
Muhammad Saleem ( Department of Haematology and Genetics, Armed Forces Institute of Pathology, Rawalpindi. )
March 1999, Volume 49, Issue 3
Original Article
Abstract
The results of a prospective study on cytogenetic analysis of Chorionic Villus Samples (CVS) taken in early pregnancy (after 10 weeks) from pregnant ladies aged between 22 and 50 years are being presented.
Objective: To find out the prevalence of chromosomal defects with advancing age of the mother. Sefting Department of Medical Genetics, Armed Forces Institute of Pathology, .Rawalpindi.
Methods: A total of 48 samples have been studied. Ten patients were above the age of 35 years and 38 were below the age of 35 years. Chorionic villus samples were obtained after 10th week of pregnancy through transabdominal approach. Cytogenetic cultures were set up both by the direct and routine methods.
Results: Three out of the seven samples taken from expecting mothers aged above 35 and one culture from a patient aged less than 35, showed trisomy 21.
Conclusion: This study highlights the fact that incidence of chromosomal aberrations and the Down’s syndrome in particular, increases with the advancing maternal age. Prenatal studies can therefore be utilized to decrease the incidence of various chromosomal abnormalities (JPMA 49:60, 1999).
Introduction
Babies born with Down’s syndrome (trisomy 21), being mentally subnormal pose several social, psychological and financial problems to their parents. In addition they carry an increased risk of multiple congenital abnormalities including those of cardiovascular, gastrointestinal and musculoskeletal system1 and there is also an increased incidence of developing several malignant disorders2 which further aggravate the misery of the family. Overall incidence of Down’s syndrome has been reported as 1/700 live births3. However, the risk of Down’s syndrome increases with the advancing age of the pregnant mothep4.
Recent advances in the techniques of obtaining samples of foetal tissue, at 10-12 weeks and improved methods of analyzing karyotype of the foetus from these samples has made it possible to detect the various chromosomal abnormalities early in pregnancy2. Antenatal diagnosis makes a safe therapeutic abortion possible, thus preventing the birth of an abnormal baby. As a matter of fact it is highly recommended to perform such procedures in all pregnancies occurring after the age of 35 years5.
There is an increased chance of detecting trisomic fetal karyotype by prenatal cytogenetic studies at an earlier stage of pregnancy than at full term because a proportion of Down’s syndrome pregnancies are lost spontaneously during the 1st or 2nd trimester6.
To practice such preventive measures it is important that required awareness exists in the population concerned and there is enough expertise to perform the procedure safely and accurately. In the past few years, at least the educated people in Pakistan have become aware of the well recognized association of advancing maternal age and the increased risk of Down’s syndrome and other trisomic syndromes. No standard criteria exists for exact maternal age for offering the option of an invasive techniques for fetal chromosomal analysis. Most centers routinely offer prenatal diagnostic option to women over 35 years of age7.
This report is based on foetal tissue obtained from pregnant ladies with advanced age specifically referred by the gynecologists to the Department of Medical Genetics at Armed Forces Institute of Pathology, Rawalpindi for the antenatal diagnosis of numerical and structural chromosomal abnormalities.
Material and Methods
A total of forty-eight pregnant ladies with age ranging between 22-50 years were referred to the Department of Medical Genetics, AFIP, Rawalpindi. Chorionic villus samples (CVS) were taken by transabdominal approach under the ultrasound guidance after the 10th week of pregnancy8. Patients were divided into two groups I and H, depending on the maternal age. Group I included all those patients whose age was above 35 years and the CVS was carried out mainly to screen for Down’s syndrome and other trisomic syndromes. Group II included patients under 35 years of age. All the patients of group II underwent chorionic villus sampling to rule out various structural and numerical chromosomal abnormalities including Down’s syndrome in the conceptus.
The samples were taken in sterile normal saline. Foetal tissues were clearly dissected out under a dissecting microscope using pointed forceps and needle and the cultures were set up immediately. The samples which were required to be transported to AFIP were collected in heparinised transport medium containing basal medium such as RPMI-1640 (Sigma, UK), foetal calf serum (Flow, Scotland) and L-Glutamine (Sigma, UK), alongwith antibiotics and antifungal drugs to decrease the chances of bacterial growth9. The samples were processed as soon as they arrived in the department.
CVS cultures were set up both by direct and short term techniques. In direct culture technique, about 10 mg of chorionic villi were incubated at 37°C overnight in a medium comprising RPM! - 1640 (Sigma UK), foetal calf serum (Flow, Scotland), L-Glutamine (Sigma, UK) and 0.05 ml of colcimed (0.05 mcg/ml). Penicillin (5000 lU/mi) and Streptomycin (5000 ug/mI) were added to prevent bacterial contamination. Then the culture medium was carefully removed and villi were placed in 1% solution of sodium citrate for 10-15 minutes. Later on three washings were given with freshly prepared fixative comprising three parts of methanol and one part of glacial acetic acid. The villi were then exposed to decreasing concentrations of methanol (from 100% to 25%). A drop of 70% glacial acetic acid was placed over a slide kept on the hot plate at 40°C. A part of treated villus was kept for about four to five minutes in that drop of glacial acetic acid so that the cell dissociation was maximal from the villus. Then it was pulled up and down the slide by a sharp forceps, so that the cells got ruptured and chromosomes released. Later on one of the slide was stained with Giemsa stain to see the quality and quantity of metaphaseal spreads. Rest of the slides were exposed to dilute trypsin sol (Difco, USA) 25 mg in 100 ml of phosphate buffered saline, for about 40 seconds after ageing them at 90°C for one hour. The slides were washed immediately in distilled water and stained with Giemsa stain9.
In short term cultures, the villi were added to the medium already discussed with the difference that colcimed was added after an incubation of 24 hours at 3 7°C. Rest of the harvesting procedures were the same as that for direct dealing2. At least 20 metaphases were analyzed in detail before declaring the specimen having normal or abnormal constitutional make up.
Chi square tests were used to identify significant differences among the two groups. P value < 0.005 was considered to be statistically significant.
Results
CVS samples of 48 patients were analyzed for chromosomal abnormalities. Age of the patients ranged from 22-50 years. With the median age of 32 years and mean age of 29.3 years. Ten of our patients were above the cut off limit of 35 years (Group 1) where as rest of 38 patients were below the 35 years of age (Group II). Twenty-seven patients gave previous history of an abortion each in 1St trimester. Consanguinity was detected in forty one cases. Twenty eight of them were first cousins where as thirteen of the couples were close relatives. In group I, three women were doctors, one was a nurse, one banker and one business woman while the remaining four were house wives. In group H, three ladies were teachers while rest of thirty-five were house wives.
Two patients reported loss of the pregnancy following chorionic villus sampling after having backache and heavy vaginal bleed. Rest of the patients did not develop any major complication. Minor vaginal bleeding occurred in twelve patients where as six of them complained of backache which responded to analgesics and rest. None of the patients except one required hospital admission.
Cytogenetic studies of group I showed trisomy of G Group i.e., of chromosome #21 (Figure 1)
in three cases. Two samples showed trisomy in all the metaphases whereas one sample revealed mosaic finding of 46, XY/47, XY +21. Pregnancy was allowed to progress further till 20th week when analysis of foetal blood sample proved the diagnosis of mosaic Down’s syndrome in the foetus. In group II, only one sample revealed the presence of trisomy 21. Other abnormalities which were detected included trisomy 18 and deletion of short arm of chromosome 5 in one patient each (Table I).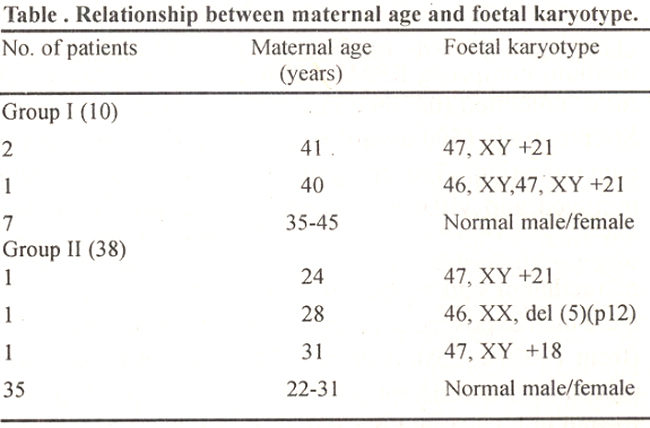
Statistical analysis of group I patients by Chisquare test revealed p value of 0.0162 indicating significantly higher frequency of Down’s syndrome in patients older than 35 years of age.

Discussion
Down’s syndrome phenotype results from the trisomy of chromosome 21, a G group autosomes. It is the most common trisomic state in human being10 Trisomy is usually caused by failure of separation of one of the pair of homologous chromosomes during the prophase of meiosis1. This condition is known as non-disjunction. The exact cause of non-disjunction is not clear. The most likely explanation is the ageing effect on the primary oocyte which can remain in a state of inactivation in dictotyene stage until the meiosis is completed at the time of ovulation when a single secondary oocyte is formed8. A very long interval between the onset of meiosis and its eventual completion, up to 35-40 years, accounts for well documented increase in the chromosomal abnormalities in the off spring of older mothers11. It is suggested that the aging causes damage to cell spindle formation and its repair mechanisms, so predisposes to non-disjunction12.
Another explanation for the association of advancing maternal age with increased risk of autosomal trisomy is that survival of trisomic embryos could be due to the age related reduction in “Immunological” competence for trisomic pregnancies in older mothers5.
In mammals radiation and delayed fertilization after ovulation do cause non-disjunction resulting in increased incidence of aneuploid embryos. It may also be of a causal relationship between maternal age and the incidence of Down’s syndrome, as with advancing age, intercourse happens less frequently resulting in delayed fertilization2.
In any case the relationship of maternal to the increased incidence of live birth of babies with Down’s syndrome is well documented1,13,14. A sharp rise starting from age 35 is observed. The incidence is even higher if the elderly mothers are subjected to prenatal cytogenetic studies early in pregnancy (10-12 weeks). This is because trisomic conceptus is more likely to be lost following intrauterine death of the foetus than a normal conceptus. Thus looking through the three parameters of chorion villus sampling around 10th week, amniocentesis around 14th week and at full term - the frequency of chromosomal abnormalities, for a particular maternal age progressively reduces15. Almost one third of the trisomic conceptus are expected to be aborted in the first trimester of pregnancy7.
The interpretation of metaphases in chorionic villus cell preparations is fairly straight forward in majority of cases as almost all the metaphases reveal either a normal karyotype or the evidence of some trisomy and the result is quite clear. In 1-2% of cases the results are rather problematical and mosaic karyotype of normal and abnormal are revealed such as 46, XX! 47, XY +21. In such cases the cytogenetic studies should be repeated on another foetal tissue such as fetal blood for confirmation and to rule out other conditions such as confined placental mosaicism16. This result from an abnormality in mitosis at an early stage of development and causing varied karyotypes in embryo and the extra embryonic tissues1.
This study suggests that the incidence of Down’s syndrome may be fairly high in pregnancies where maternal age is more than 35 years even in Pakistani ladies as three out of the seven samples from Group I revealed the trisomy 21 in only one sample from group II patients. In this family there was already a baby with Down’s syndrome. Later on cytogenetic studies of the parents revealed Robertsonian translocation involving chromosome 14 and 21 in all the metaphases in the mother. During meiosis a cell having Robertsonian translocation, can produce daughter cells either having extra chromosomal material or having lesser chromosomal number. These daughter cells, upon fertilization with a normal sperm can produce either a cell having trisomy of affected chromosomes or having monosmy of that group of chromosomes17.
Statistical analysis by Chi square test revealed p value of 0.0162. It shows a very significant risk of rising incidence of Down’s syndrome with increasing maternal age. Our study highlights the importance of cytogenetic studies on chorionic villus samples obtained early in pregnancy so that the birth of abnormal babies can be prevented by inducing therapeutic abortion. This data also reveals that the awareness for the existence of such diagnostic facilities, at the moment is mostly confined to literate couples as majority i.e., six of our patients in group I were professional ladies who themselves requested for the CVS. It therefore,, underlines the importance of organized awareness compaign to prevent the disorders causing life long miseries for both the affected child “and parents.
References
1. Falik B, Korenberg JR. Schrech RR. Confined placental mosaicism: Prenatal and postnatal cytogenetic and molecular analysis and pregnancy outcome. Am. J. Med. Genet., 1994;(1):50:51-6.
2. Muller F, Robert-Young D. Emery’s elements of medical genetics. 9th ed,, Edinburgh, Churchill Livingstone, 1995, pp.23-44.
3. Hecht CA, Hook EB. The imprecision in rate of Down’s syndrome by I-year maternal age intervals: A critical analysis of rates used in biochemical screening. Prenat. Diagn., 1994; 14:729-38.
4. Sohat M, Leguin C, Romen Y, et al. Downs syndrome prevention program in a population with an older maternal age. Obstet. Gynaecol., 1995;85:368-73.
5. Krajewska-walasek M. Maternal age downs syndrome (trisomy 21) in light of current knowledge. Pol. Tyg. Lek, 1993; 19:48:386-88.
6. Hook EB, Cross PK, Jackson L, et al: Maternal age-specific rates of 47, +21 and other cytogenetic abnorinalities diagnosed in the first trimester of pregnancy in chorionic villus biopsy specimens: Comparison with rates expected from observations at amniocentesis. Am. J. Hum. Genet., 1988;42:797-807.
7. Hook EB. Downs syndrome epidemiology and biochemical screening. In “Screening for Downs syndrome” (Grudzinskas, JG, Chard 1, Chapman M, Cuckle H eds). Cambridge University Press, Cambridge, 1994, pp. 1-18.
8. Ellis AR. Antenatal screening for Down’s syndrome. Can we do better. Ann. Clin. Biochem., 1993;30:421-24.
9. Rooney DE, Gzepulkowski BH. Human cytogenetics. A practical approach. Vol.1, Oxford IRL Press, Oxford University Press, 1992, pp. 75-84.
10. Salonen R, Sirnola KO, Harjulehto T, et al. Incidence of Down’s syndrome and non disjunction of chromosome 21 in maternal meiosis: Evidence for a matemal age dependent mechanism involving reduced recombination. Hum. Mol. Genet., 1994;3:1529-35.
11. Alfi OS, Chang R, Azen P. Evidence of genetic control of non-disjunction in man. Am. J. Hum. Genet., 1980;32:477-83.
12. Rushton Dl. Examination of the products of conception from previable human pregnancies. J. Clin. Pathol. 1981:34:819-35.
13. Cooley WC, Graham JR. Down’s syndrome - An update and review for primary pediatricians. Clin. Pediatr., 1991;30:233-53.
14. Hanan A, Hamamy Zuhaair S. Al-Taha S. Consanguinity and the genetic control of Down’s syndrome. Cliii. Genet., 1990;37:24-29.
15. Halliday JL, Watson LF, Lumley J, et al. New estimates of Down syndrome risks at chorionic villus sampling, amniocentesis and live birth in women of advanced maternal age froni a uniquely defined population. Prenat. Diagn., 1995;1 5:455-65.
16. Sitnoni G, Sirchia SM. Confined placental mosaicism. Prenat. Diagn., 1994;14:1 185-89.
17. Ucimida IA, Freeman VCP. Trisomy 21, Down syndrome and structural chromosomal abnormalities in the parents. Hum. Genet., 1986;72: 118-22.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: