
Qurratulain Hyder ( Departments of Gastroenterology & General Surgery, Pakistan Institute of Medical Sciences (PIMS), Islamabad, Pakistan. )
Mohammad Ahmad Zahid ( Departments of Gastroenterology & General Surgery, Pakistan Institute of Medical Sciences (PIMS), Islamabad, Pakistan. )
Arif Malik ( Department of Surgery, Shifa International Hospitals, Islamabad, Pakistan. )
Rakhshanda Rasheed ( Departments of Gastroenterology & General Surgery, Pakistan Institute of Medical Sciences (PIMS), Islamabad, Pakistan. )
November 2011, Volume 61, Issue 11
Case Reports
Abstract
Conventional endotherapy for pancreatic pseudocyst involves placement of stents in the cyst cavity. We have successfully treated bulging pseudocyst in a 50 year old male by endoscopic incision drainage (EID), without insertion of endoprostheses. The presenting complaints in our patient were epigastric mass and postprandial vomiting. He had recently undergone open cholecystectomy following recovery from gallstone pancreatitis. EID was performed under general anaesthesia. Needle knife was advanced through the accessory channel of a flexible gastroscope. Cyst contents were evacuated by making 5 cm horizontal incision on the gastric indentation with dramatic relief in symptoms. There is no cyst recurrence during follow up for over 3 years.
Keywords: Pancreatic pseudocyst; Cystogastrostomy; Endotherapy; Natural orifice transluminal endoscopic surgery (NOTES); Endoscopic incision drainage.
Introduction
Pseudocyst of pancreas complicates 7-15% episodes of acute pancreatitis.1 The cyst communicates with main pancreatic duct (MPD) in >60% of cases.2 Percutaneous drainage of the pseudocyst is unpopular due to infection and persistent leakage from drainage site. Surgery is nearly 100% effective3 albeit with high morbidity (35%) and mortality (10%).4 The cyst wall should be adequately thick to hold sutures. Endoscopic treatment is universally regarded as minimally invasive alternative to surgery. It was introduced by Kozarek et al in 1985.5 Buchi et al reported endoscopic laser cystogastrostomy in 1986.6 Flexible peroral stapler under endoscopic guidance is used for creation of wide cystoenteric fistula.7 However, gradual and inefficient cyst drainage with endotherapy is associated with demerits, pertaining to prostheses, cost, cyst resolution and recurrence. Most of these issues can be overcome by EID, which favours prompt resolution by abruptly eliminating the necrotic debris. EID is not previously described in medical literature.
Case Report
The patient was 50 year old male, who presented with dull epigastric pain and vomiting since 12 days. There was no history of fever, jaundice and consumption of alcohol. He admitted smoking more than 40 cigarettes/day since 10 years. Five months earlier, open cholecystectomy was performed after an attack of biliary pancreatitis. Clinical evaluation revealed mild anaemia and an ill defined cystic mass in the epigastrium. Nutritional status was adequately preserved. Laboratory investigation showed: total leukocytes: 9000/mm3 (polymorphs: 70.20%; lymphocytes: 22%); haemoglobin: 9.7g /dL; mean corpuscular volume: 81.8 fl; platelet count: 661000/mm3; erythrocyte sedimentation rate: 37 mm/Ist hour; serum bilirubin: 1.6 mg/dL; serum alanine aminotransferase (ALT): 18 IU/L; serum alkaline phosphatase (ALP): 298 IU/L; Prothrombin time: 17 s (control: 15 s); serum amylase: 172 U/L; serum lactic dehydrogenase: 1074 U/L; blood glucose: 97 mg/dL; blood urea nitrogen: 47 mg/dL; serum creatinine: 1.4 mg/dL; serum K+: 4.3 mEq /L; serum Na+: 135 mEq/L and serum Ca++: 8.5 mg/dL. Screening for hepatitis B and C was negative. Urinalysis was normal. Chest radiograph showed hyperlucent lungs with atelectatic bands in both lower zones and blunting of the right costophrenic angle. Abdominal sonography revealed a large, thick walled, unilocular cyst anterior to head and body of the pancreas. It measured 12.7 x 10.8 cm in diameter and demonstrated internal echoes. On computed tomography (CT) scan, gastric encroachment by the pseudocyst appeared as indentation of posterior wall of the antrum (Figure-1).
Gastric convexity was grossly visible on endoscopy.
EID was performed under general anaesthesia on 7th November, 2007 after obtaining informed consent. Surgical team was standby for an urgent situation. Intravenous antibiotics were initiated 12 hours before the procedure. The most convex part of antral indentation was punctured with a needle knife passed through flexible endoscope. Spurting of necrotic material confirmed access to the cyst cavity (Figure-2A).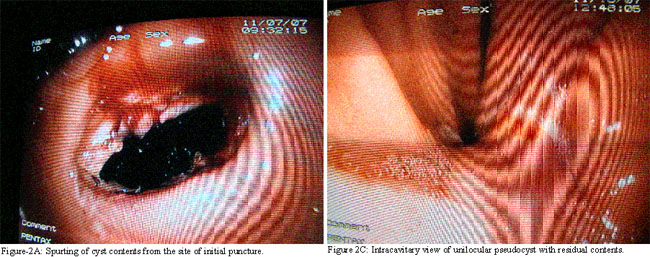
A large cystogastrostomy was created by 5cm long needle knife incision across the site of initial puncture (Figure-2B).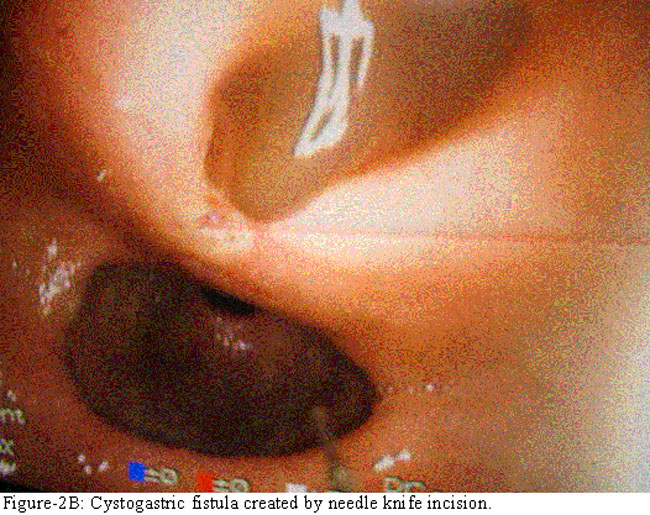
Abrupt evacuation of >500ml tarry contents coincided with collapse of the antral convexity and mass in the epigastrium. Cyst cavity was examined for residue, septations and neoplasm (Figure-2C).The procedure time was 15 minutes. Nasogastric output was approximately 800 ml in 48 hours postoperatively. Vital signs and haemoglobin remained stable during one week indoor observation. Parenteral alimentation, antibiotics and proton pump inhibitors were discontinued on day 5. Cystogastric fistula had nearly closed on day 6 (Figure-2D) and it was barely visible on interval endoscopy after 3 weeks. CT scan of the abdomen could not be repeated due to refusal by the patient.
Discussion
Endoscopic treatment of pseudocysts has significantly reduced morbidity and pain associated with surgery. It is now utilized for the management of pancreatic abscesses.8 The endoscopic method, however, has several disadvantages. Cyst recurrence is not uncommon due to slow and incomplete emptying of pseudocysts after endotherapy. Insertion of prostheses requires long term antibiotic prophylaxis. These devices need to be frequently replaced due to occlusion, migration, kinking and perforation. Deployment of covered metal stents or multiple stents is sometimes necessary to ensure efficient drainage because minimal debris escapes between the clogged prostheses. Cyst emptying is further compromised in multilocular and communicating pseudocysts. We have circumvented these problems by creating a large endoscopic fistula on the principle of NOTES. The end result is similar to surgical cystogastrostomy though with minimal trauma and morbidity. Care was exercised to avoid peripheral extension of needle knife incision, which may cause gastric perforation (Figure-3).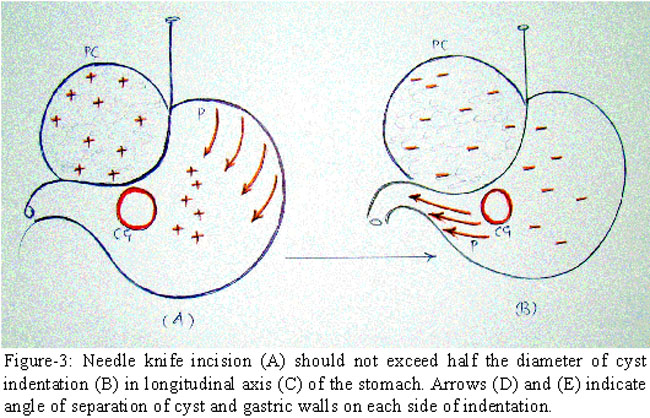
By eliminating the use of stents, EID seems to reduce cost of procedure and prevent complications due to prostheses. No recurrence of cyst in the present case augments our belief that more rapid and near total evacuation of the cyst is feasible with EID than with endoprostheses. Abrupt removal of necrotic material and pancreatic juices appears to facilitate cyst resolution and bridging of the MPD. Gastric contractions and relaxations further promote cyst clearance by transmitting pressure changes to the cyst cavity (Figure-4AB).
This hypothesis is supported by an early collapse of pseudocyst in our patient. EID permits direct inspection of cyst cavity for septations and mass lesion e.g. cystic tumours of pancreas. The risk of haemorrhage with endotherapy is 6%.9 Most of the bleeding etiologies are preoperatively detectable. The interposed blood vessels are stretched and partly occluded due to enlargement of cyst. Blended current coagulates these vessels and fuses walls of the stomach and pseudocyst along the line of cystogastrostomy. Thus risk of bleeding during EID is apparently low. This perception is reinforced by stability of clinical and laboratory parameters as in the present case. Endoscopic ultrasound (EUS) provides major breakthrough in the diagnosis of cystic neoplasms and treatment of no-bulging or infected pseudocysts. However, EUS requires a "sequential approach" with ultimate reliance on flexible endoscopy for placement of endoprostheses in the most dependent part of pseudocyst.10 On the contrary, desired angle of access is conveniently achieved during EID. By virtue of prompt cyst drainage, both communicating and non-communicating pseudocysts may respond equally to EID. Endoscopic retrograde cholangiopancreatography to exclude downstream obstruction of the MPD is thus more suitable for pseudocysts, which fail to respond to EID. With availability of staplers for endoscopic interventions, we expect EID to become popular as an outdoor procedure for indenting pseudocysts.
Conclusion
We conclude that EID is a simple and cost effective procedure in selective cases. More work is required before it is widely recommended for treatment of bulging pseudocysts of pancreas.
References
1.Govil D, Khanna S, Virmani S, Jha A, Kumar S. Surgery for complicated pancreatic pseudocysts--report from a tertiary center. Indian J Gastroenterol 2004; 23: 33-4.
2.Enya M, Yasuda I, Shirakami Y, Ostugi K, Shinoda T, Moriwali H. Endoscopic ultrasound-guided drainage of pancreatic pseudocysts using a large-channel echoendoscope and a conventional polypectomy snare. Digestive Endosc 2003; 15: 323-8.
3.Parks RW, Tzovaras G, Diamond T, Rowlands BJ. Management of pancreatic pseudocysts. Ann R Coll Surg Engl 2000; 82: 383-7.
4.Giovannini M, Binmoeller K, Seifert H. Endoscopic ultrasound-guided cystogastrostomy. Endoscopy 2003; 35: 239-45.
5.Kozarek RA, Brayko CM, Harlan J, Sanowski RA, Cintora I, Kovac A. Endoscopic drainage of pancreatic pseudocysts. Gastrointest Endosc 1985; 31: 322-7.
6.Buchi KN, Bowers JH, Dixon JA. Endoscopic pancreatic cystogastrostomy using the Nd: YAG laser. Gastrointest Endosc 1986; 32: 112-4.
7.Norton ID, Clain JE, Wiersema MJ, DiMagno EP, Petersen BT, Gostout CJ. Utility of endoscopic ultrasonography in endoscopic drainage of pancreatic pseudocysts in selected patients. Mayo Clin Proc 2001; 76: 794-8.
8.Vitale GC, Davis BR, Vitale M, Tran TC, Clemons R. Natural orifice translumenal endoscopic drainage for pancreatic abscesses. Surg Endosc 2009; 23: 140-6.
9.Vazquez-Sequeiros E. Drainage of peripancreatic-fluid collections: is EUS really necessary? Gastrointest Endosc 2007; 66: 1120-2.
10.Antillon MR, Shah RJ, Stiegmann G, Chen YK. Single-step EUS-guided transmural drainage of simple and complicated pancreatic pseudocysts. Gastrointest Endosc 2006; 63: 797-803.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: