
Syed Rehan Ali ( Department of Pediatrics and Child Health, The Aga Khan University Hospital Karachi, Pakistan. )
Maqbool Qadir ( Department of Pediatrics and Child Health, The Aga Khan University Hospital Karachi, Pakistan. )
Shakeel Ahmed ( Department of Pediatrics and Child Health, The Aga Khan University Hospital Karachi, Pakistan. )
Prem Kumar ( Department of Pediatrics and Child Health, The Aga Khan University Hospital Karachi, Pakistan. )
November 2011, Volume 61, Issue 11
Case Reports
Abstract
Foetus-in-foetu is a rare malformation in which a monozygotic diamniotic parasitic twin is incorporated into the body of its fellow twin and grows inside it. Less than 100 cases have been reported in literature. One day old newborn male was admitted with antenatal diagnosis of abdominal mass. It was cystic/solid in nature with pressure effects on left ureter and urinary bladder, most likely to be a germ cell tumour. Birth history was uneventful. Exploratory laparotomy was performed and the mass was excised. Physical examination confirmed the diagnosis of foetus-in-foetu. Although it is a rare condition, imaging may play an important role in the correct prospective diagnosis of foetus-in-foetu. Surgical excision is the recommended treatment.
Keywords: Foetus-in-foetu, Abdominal mass.
Introduction
The term foetus-in-foetu was first described by Meckel (circa 1800) and the first reported case was cited in 1809 by Young.1 The term foetus-in-foetu is used to point out an unequal division of totipotential cells of a blastocyst which results in the inclusion of a small cellular mass in the more mature embryo. This is a form of monozygotic diamniotic twin pregnancy where the parasitic twin installs and grows in the body of its partner.2
Foetus-in-foetu is a rare entity.3 The incidence is about 1:500,000 deliveries and less than 100 cases have been reported in literature.3 The majority of cases occur are diagnosed in infancy and/or very rarely in older age.4
In 70% of cases the chief complaint is an abdominal mass.5 It is predominantly seen retroperitoneally in 80% of cases but can present at atypical sites like the skull, sacrum, scrotum and the mouth. Eighty-nine per cent of foetus-in-foetu lesions were noted before 18 months of age.1,5,6 Tharkral et al. reported equal male and female prevalence.7
Case Presentation
One day old newborn male was admitted in Neonatal Intensive Care Unit (NICU) with antenatal diagnosis of a cystic/solid abdominal mass with pressure effects on left ureter and urinary bladder, most likely to be a germ cell tumour. Birth was uneventful. Baby underwent exploratory laparotomy on the 3rd day of life and the mass was successfully excised. Perioperative findings showed a well-circumscribed mass in left retroperitoneal region with left ureter matted to the posterior wall and also to the descending colon. Foetus-in-foetu with umbilical cord arising from the amniotic sac was identified with partially developed rudimentary lower limbs (Figure-1 and 2).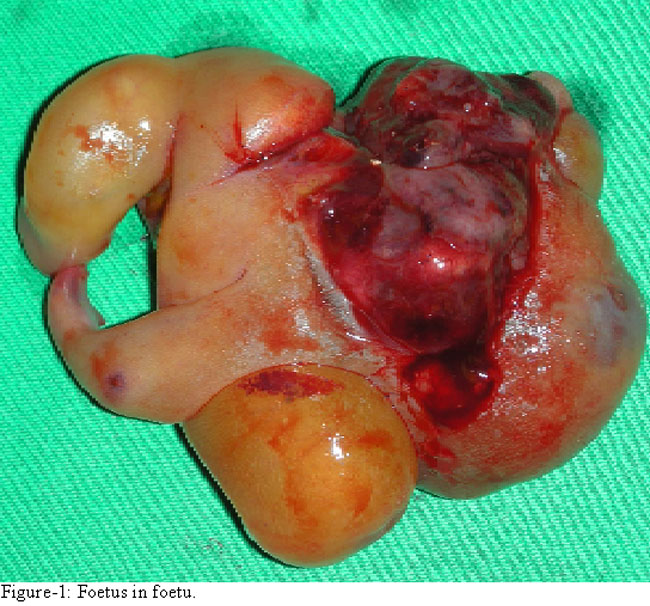

Histopathology findings were consistent with foetu-in-foetu. Post surgery course was uneventful. Baby remained in hospital for 5 days and was discharged on feeds.
Discussion
Foetus-in-foetu is a condition where a malformed twin is found inside of the body of its co- twin. It can be located at any site in the body. The term foetus-in-foetu is used to draw attention to an unequal division of totipotential cells of a blastocyst which results in the inclusion of a small cellular mass in the more mature embryo. This is a form of monozygotic diamniotic twin pregnancy where the parasitic twin installs and grows in the body of its partner.2
This is a rare malformation that has some similarities with retroperitoneal teratoma, but it is different from the latter by its fetiform aspect and the metameric segmentation of its spinal axis.2 However, not all reported cases of foetus-in-foetu have an identifiable spine.8-10
The differential radiologic diagnoses are teratoma and meconium pseudocyst. Indeed, these masses often have had calcified components, so they have been sometimes difficult to differentiate with foetus-in-foetu.6
In reviewing literature most case reports up till 1980 showed that preoperative diagnosis of foetus-in-foetu was made only in 16.7% of cases because CT scan was not performed. Nowadays, CT scan has proven to be very helpful in suggesting the preoperative diagnosis.11
Although there has been little evidence of organogenesis in literature, mature somatic tissue from ectodermal (neuroepithelium, ganglia), endodermal (colon) and mesodermal (bone and cartilage) origins have been present. These, together with the presence of a complete vertebral column with appropriate arrangements of limbs around it, differentiate foetus-in-foetu from a teratoma. Complete excision of the surrounding membrane, should make certain of an unambiguous cure.12
Hopkins et al reported malignant recurrence following resection of a foetus-in-foetu.3 This was presumably caused by transformation of adherent membranes remaining at the surgical site. In view of this report, early and frequent post operative followup is recommended, especially if the sac cannot be completely resected. This may be achieved with moderate sensitivity using serum tumour marker concentration or by regular imaging.3
Conclusion
Foetus-in-foetu is a very rare and extraordinary condition. CT scan or MRI may play a vital role in its correct antenatal diagnosis. Although rare, the tumour should be removed for confirmation of diagnosis and its potential effect on normal renal function and its trivial malignant potential.
References
1.Fetus in Fetu: A Case Report and Literature Review. Pediatrics 2000; 105: 1335-44.
2.Kaufman D, Du L, Velcek FT, Alfonso AE. Fetus in Fetu. J Am Coll Surgeons 2007; 205: 378-9.
3.Hopkins KL, Dickson PK, Ball TI, Rickett SRR, O\\\'Shea PA, Abramowsky CR. Fetus in Fetu with malignant recurrence. J Pediatr Surg 1997; 32: 1476-9.
4.Senyüz OF, Rizalar R, Celayir S, Oz F. Fetus in fetu or giant epignathus protruding from the mouth. J Pediatr Surg 1992; 27: 1493-5.
5.Kakizoe T, Tahara M. Fetus in fetu located in the scrotal sac of a newborn infant: a case report. J Urol 1972; 107: 506-8.
6.Sanal M, Kucukcelebi A, Abasiyanik F, Erdogan S, Kocabasoglu U. Fetus in fetu and cystic rectal duplication in a newborn. Eur J Pediatr Surg 1997; 7:120-1.
7.Thakral CL, Maji DC, Sajwani MJ. Fetus in fetu: a case report and review of literature. J Pediatr Surg 1998; 33: 1432-4.
8.Du Plessis JPG, Winship WS, Kirstein JD. Fetus in fetu and teratoma. S Afr Med J 1974; 48: 2119-22.
9.Eng HL, Chuang JH, Lee TY, Chen WT. Fetus in fetu: a case report and review of literature. J Pediatr Surg 1989; 24: 269-9.
10.Willis RA. The borderland of embryology and pathology. 2nd ed. Washington DC: Butterworth 1962; pp 442-62.
11.Tsai CH, Lin JS, Tsai FJ. Intraventricular fetus in fetu: report of one case. Acta Paediatr Sin 1993; 34: 143-50.
12.Lewis RH. Fetus in Fetu and retroperitoneal teratoma. Arch Dis Child 1960; 36: 220-6.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: