
Mohammad Naeem ( Department of Community Medicine, Peshawar. )
Muhammad Zia-ul-Islam Khan ( Student of Final year MBBS, Peshawar. )
Syed Hussain Abbas ( Student of Final year MBBS, Peshawar. )
Muhammad Adil ( Student of Final year MBBS, Peshawar. )
Muhammad Usman Khan ( Khyber Medical College. Khyber Teaching Hospital, Peshawar. )
Syeda Maria Naz ( Khyber Medical College. Khyber Teaching Hospital, Peshawar. )
November 2011, Volume 61, Issue 11
Short Reports
Abstract
Hepatitis B is a major burden in Pakistan. A cross-sectional study was conducted in Peshawar, from 9th June to 19th June 2010. Cluster random sampling was done. Confidence level of 95% and confidence interval of 5 was used to derive sample size. Parents of 506 children were asked about their hepatitis B immunization status who were aged 4 years or under. Questions on demographics, income, education, accessibility and occupation, knowledge and views on immunization were asked. Forty health personnel were interviewed for their views.
In all, 62.2% children were completely vaccinated. Reasons for not being immunized included unawareness, busy schedule, long distance to the centre and various misconceptions. Education, mothers\\\' knowledge and views on immunization, income, closer accessibility, were the main factors associated with immunization. Health personnel thought lack of awareness among people, low accessibility and poor incentives as the shortcomings in immunization. It is recommended that effective steps should be taken to ensure better coverage.
Keywords: Hepatitis B, Childhood immunization, Peshawar.
Introduction
Hepatitis B causes both acute and chronic liver disease. About 2 billion people have been infected all over the world, 350 million people live with chronic infection, an estimated 600,000 people die every year due to acute or chronic Hepatitis B and about 25% of adults infected during childhood, will eventually die of the disease.1 Although Hepatitis B has high morbidity and mortality yet it is preventable with an effective and safe vaccine.1
In areas where mother-to-infant spread of Hepatitis B Virus (HBV) is common, the first dose of vaccine should be given as soon as possible after birth. In Pakistan however, Hepatitis B is given at 6th, 10th and 14th week respectively.
Hepatitis B vaccination is crucial as Pakistan carries one of the world\\\'s highest burdens of chronic hepatitis and mortality due to liver failure and hepatocellular carcinomas. National level estimates of the prevalence for Hepatitis B is 3-4%.2 The purpose of this study is to assess the situation in the most developed part of Khyber-Pakhtunkhwa - Peshawar. This study seeks to find the factors influencing vaccination coverage and non immunization with respect to the user as well as the provider and to compare these findings with other relatively developed semi- urban parts of Pakistan in order to provide new material for any future approaches to Hepatitis B vaccination to attain better immunization results.
Methods and Results
A cross sectional study was conducted from 9th to 19th of June 2010 in Peshawar. Two-stage cluster random sampling was done. The areas where households were interviewed were Peshawar university campus, Hashtnagri, Naway Kalay and Pawaka village. A researcher-administered standard questionnaire was used as a data collecting tool in which parents were asked about their children\\\'s Hepatitis B immunization status, demographics, education status, occupation and income. Information regarding immunization, accessibility to health centres and parents\\\' views on immunization was also taken. A confidence interval of 5 and confidence level of 95 % was used to derive the sample size. All data was collected through informed consent from parents of 506 children, aged 4 years or under. Infants less than 6 weeks and children who had not spent their immunization life time (1st year of life) in Peshawar were excluded. The reason for taking 4 years as cut off limit was to assess the situation in children and get a broader scope of performance of Immunization programme. Immunization record was noted through cards if present or through memory recall. Forty health personnel were also interviewed in different immunization centres of Khyber Teaching Hospital, Lady Reading Hospital and different BHUs. A separate questionnaire containing demographic data, questions about main hurdles in vaccination, their access to vaccines, its quality, cold chain equipment, salaries and special incentives was used. All data was analyzed using SPSS 16.0. Pearson\\\'s chi-square test was used for testing the significance of relation between variables. A P value of < 0.05 was considered significant.
Out of 506 children 264 (52.2%) were females and 242 (47.8%) were males. Urban population was 54.3%. The immunization coverage against Hepatitis B was; 62.2% completely vaccinated, 19.6% incompletely vaccinated and 18.4 % were not vaccinated. For 1st dose 81.6%, 2nd dose 68.2 % and 3rd dose 62.2% were vaccinated.
The reasons for not being vaccinated were lack of awareness (26.1%), family problems or busy schedule (21.6%), long distance to centre (19.1%), misconceptions (8.5%), child being ill (7.5%) and fear of reactions (1.0%). Immunization card were available with 53.0% parents.
Most of the parents had little knowledge on importance of vaccination (32.8%), a significant number had no knowledge at all (12.3%) and very few knew everything important about immunization (6.9%). When asked whether the immunization programme was beneficial, 90.9% answered yes. Negative answers were 9.1% (n=46). The reasons behind this were; fear of reactions (30.4%), thoughts about immunization not being effective (30.4%), having wrong ideas about vaccines e.g. it being a case of sterility (21.7%) and previous bad experiences (8.6%).
Cross tabulation between education of parents and the immunization is shown in Figure-1.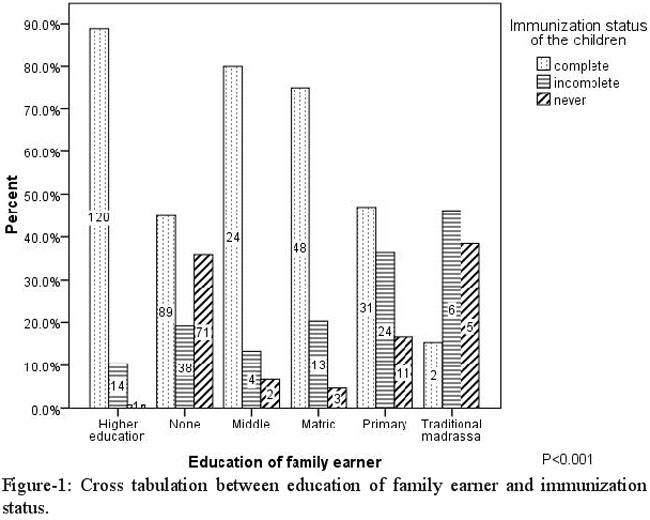
Mothers who had enough knowledge on immunization, had 89.7% of children immunized as compared to 27.4% with no knowledge at all (P <0.001). High immunization rates were found for urban areas (74.2%) in comparison to rural areas (47.6%) (P <0.001). A significant pattern was not observed with respect to sex of the child (males 61.2% and females 62.9%, P 0.716).
Immunization was high for household earners having government (69.8% immunized) and private jobs (76.7% immunized) rather than labourers (41.8% immunized) (P <0.001). The income had a great effect on the immunization status of the child (Figure-2).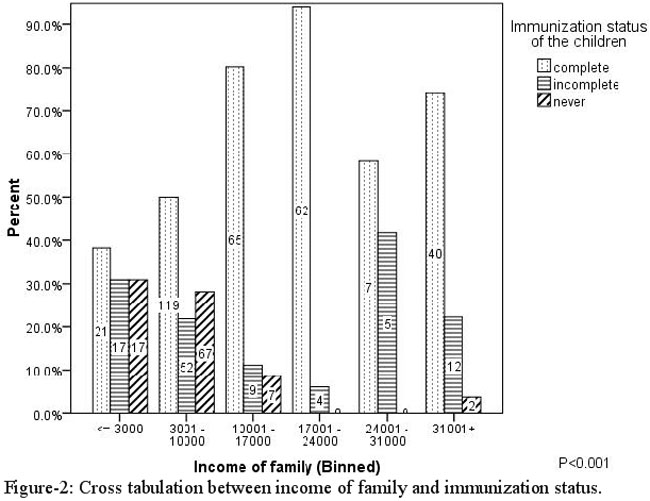
A small progressive fall was seen in immunization with increase in distance from vaccination facilities. However, a large decrease was observed beyond 11km (P <0.001).
All the health workers quoted to have had training and knew how to handle the cold chain. Adequate equipment for the cold chain was also available. Most were not satisfied with the salaries and incentives (70%). Main difficulties were; lack of awareness among people (32.5% n=13), load shedding (20% n=8), negative role of media (7.5% n=3), security problems (10.0% n=4), transportation problems (10% n=4) and lack of vaccines (10.0% n=4).
Discussion
The full immunization coverage was similar to the 2006-07 Demographic and Health Survey report.3 This study showed better results than other parts of Khyber-Pakhtunkhwa.4 The reasons could be that Peshawar is an urban area, which usually has higher coverage than rural areas.5 Studies in other countries show similar results. Causes of low vaccination were similar to studies of Khyber-Pakhtunkhwa4 and elsewhere.6,7
Low immunization was seen among families with uneducated and low earning parents and vice versa. It was also noted that mothers having knowledge about immunization and its importance had much greater immunization rates for their children.4 This shows clearly the impact of education of both parents on immunization, stressing the importance of education in success of immunization. An important study in Taiwan, which represents a country with a success story regarding Hepatitis B vaccination showed similar results.6
A significant pattern was not observed regarding sex in studies conducted elsewhere.8 The reason behind this could be that social factors regarding sex do not come to play in children at such a young age especially when it comes to availing free services like immunization.
Immunization was high for government and private jobs rather than labourers probably due to income disparities between them.6 The income of family and the immunization status had a very clear relationship. This was consistent with other studies.5,7,9 Income of family plays a role in availing free services like immunization because of reasons like lack of time by the caretaker, Poor accessibility, social depravity and poor education were other important factors. One of the main causes of low vaccination was the distance of a functional vaccination centre. A clear relationship didn\\\'t exist below 11 km. However, above 11km there was a sharp decrease in immunization. This relation was not uncommon.4,7 Therefore, a need for improvement in access to health centres is needed.
Most of the mothers thought vaccination was useful but significant number did not consider it useful (8.8%), indicating the need for health education.7 Measures are required to eliminate such misconceptions, if any meaningful progress is to be made in immunization.
All the health workers quoted to have had training and knew how to handle the cold chain. They also had adequate equipment for cold chain. This was in contrast to studies conducted in Pakistan.10 Problems faced by health workers are quite similar to other studies. Major problems like no awareness, transport and load shedding have to be addressed, salary structure should also be improved to increase their efficiency.7,10
Several methodological issues and limitations have to be considered regarding this study. First, the cross sectional nature of the study does not permit an interpretation of clear causal relation. Second, the study was conducted in Peshawar which attracts a significant amount of immigrants from other parts of the province and especially under privileged Afghan migrants, which can as a whole affect the outcomes in this study.
Conclusion
Immunization status and coverage for Hepatitis B in Peshawar is very low. Lack of awareness and low accessibility, associated with low literacy and poor socioeconomic conditions have to be addressed in order to improve immunization. The health workers face difficulties like lack of awareness, load shedding, transportation and security. Lack of incentives also appears to be a reason for the low performance of immunization staff.
References
1.WHO. Hepatitis B Fact sheet. (Online) (Cited 2010 June). Available from URL: http://www.who.int/mediacentre/factsheets/fs204/en/.
2.Ministry of health, Expanded Program on Immunization (EPI). (Online) (Cited 2010 June). Available from URL: http://www.health.gov.pk.
3.Pakistan demographic and health survey 2006-2007. Chapter 10, Child health. (Online) (Cited 2010 June). Available from URL: http://www.measuredhs.com/pubs/pdf/FR200/FR200.pdf.
4.Ahmad N, Akhtar T, Roghani MT, Ilyas HM, Ahmad M. Immunization coverage in three districts of North West Frontier Province (NWFP). J Pak Med Assoc 1999; 49: 301-5.
5.Fotso JC. Child health inequities in developing countries: differences across urban and rural areas. Int J Equity Health 2006; 5: 9.
6.Chin-Shyan Chen, Tsai-Ching Liu. The Taiwan National Health Insurance Program and Full Infant Immunization Coverage. Am J Public Health 2005; 95: 305-11.
7.Mansuri FA, Baig LA. Assessment of immunization service in perspective of both the recipients and the providers: a reflection from focus group discussions. J Ayub Med Coll Abbottabad 2003; 15: 14-8.
8.Corsi DJ, Bassani DG, Kumar R, Awasthi S, Jotkar R, Kaur N, et al. Gender inequity and age-appropriate immunization coverage in India from 1992 to 2006. BMC Int Health Hum Rights 2009; 9(Suppl 1): S3.
9.Mitchell S, Andersson N, Ansari NM, Omer K, Soberanis JL, Cockcroft A. Equity and vaccine uptake: a cross-sectional study of measles vaccination in Lasbela District, Pakistan. BMC Int Health Hum Rights 2009; 9 (Suppl 1): S7.
10.Mushtaq MU, Shahid U, Majrooh MA, Shad MA, Siddiqui AM, Akram J. From their own perspective - constraints in the Polio Eradication Initiative: perceptions of health workers and managers in a district of Pakistan\\\'s Punjab province. BMC Int Health Hum Rights 2010; 10: 22.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: