
F. K. Tareen ( Department of Surgery, Aga Khan University Hospital, Karachi. )
S. Hussain ( Department of Surgery, Aga Khan University Hospital, Karachi. )
F. Moazam ( Department of Surgery, Aga Khan University Hospital, Karachi. )
August 2001, Volume 51, Issue 8
Case Reports
Introduction
Thyrnic hyperplasia is the most common anterior mediastinal mass in infants and the patient is usually asymptomatic1,2. True thyrnic hyperplaisa is characterized by massive thymic hypertrophy however, the normal thymic architecture is retained3. Massive thyrnic hyperplasia (MTH), a rare variant of hyperplasia of the thymus, is known to cause mediastinal compression or acute and recurrent respiratory infections in the pediatric age group. It needs to be distinguished from other commonly seen masses of the anterior mediastinum2. We report two such cases and allude to the clinicopathological scenario in which they present and management options in these cases.
Case Report 1
A three month-old baby boy weighing 7.8 kg presented with respiratory distress, being treated for presumed pneumonia for last three weeks. Chest X-ray and CT scan revealed mass in the anterior mediastinum occupying upper half of both hemithoracis (Figure Ia, 1 b).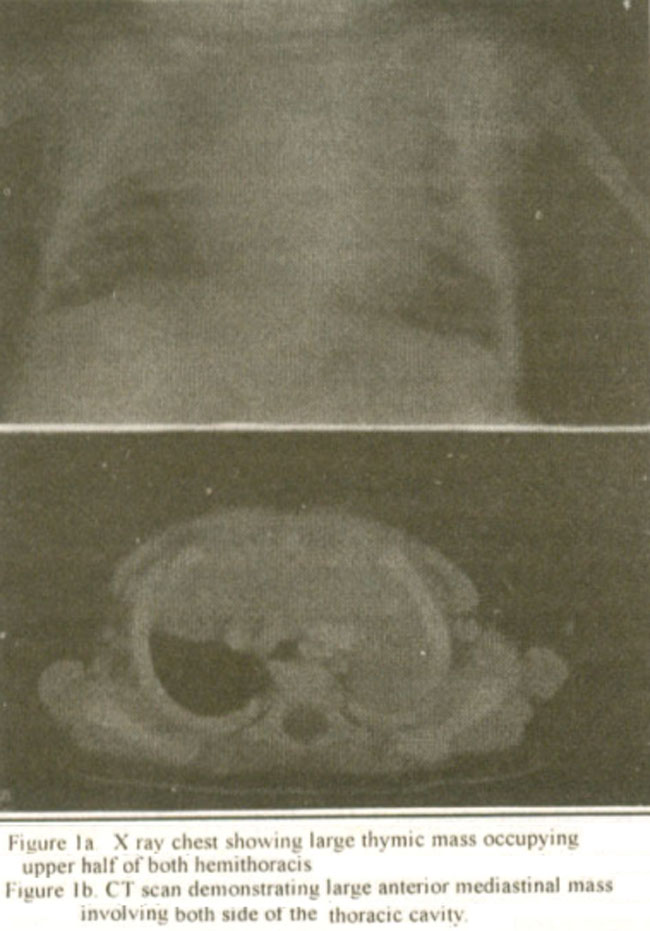
Based on clinical and radiological features, provisional diagnosis of thymic hyperplasia was made and the patient was given oral steroids. The child showed marked clinical improvement within a week. Subsequent follow up with ultrasound scan and X-ray chest showed considerable reduction in size. The steroid was tapered off after one week. On subsequent follow up of over six months, there is no evidence of clinical and al relapse.
Case Report 2
An eight-month-old baby boy weighing 5.6 kg was referred for evaluation of anterior mediastinal mass. The patient had been treated for presumed respiratory infection at referring facility for the last three months. At presentation. examination revealed the child to be tachypnoeic. dyspnoeic. with intercostals recession and stridor. Chest radiograph and CT scan revealed a large anterior mediastinal mass, occupying entire right hemithorax and causing collapse of the right lung (Figure 2 a,2b).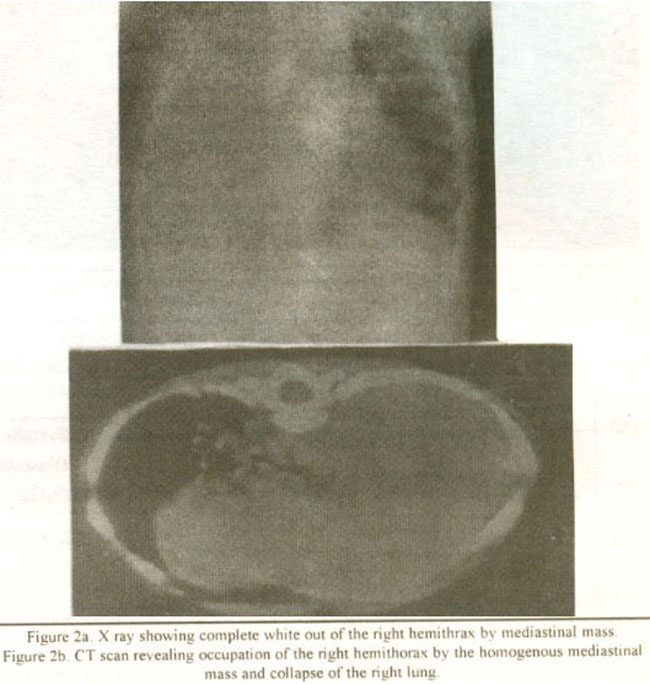
Based on clinicoradiological features, diagnosis of thymic hyperplasia was made and on oral steroids started.
After initial remission, symptoms relapsed. CT guided fine needle aspiration biopsy (FNA) showed mature thymic cells with Hassal’s corpuscles. Thymus which occupied nearly entire hemithorax was excised. Postoperative recovery was uneventful and child on follow up over six months is asymptomatic. Histology confirmed the diagnosis ofthymic hyperplasia.
Discussion
MTH is a rare condition of abnornial thymic growth3. Thymus can be quite prominent in the newborn but very little to be seen after the age of two years4. Confusion arises to differentiate the thymic hyperplasia from both normal and abnormal condition of thymic growth.
MTH is a rare idiopathic variant of true thymic hyperplasia. Literature review showed sporadic case reports of symptomatic thymic hyperplasia. No definite criteria for diagnosis of MTH exists, but the following guidelines have been suggested for the definition of MTH2: (I) It should be greater than the heart shadow on posteroanterior chest radiograph (2) The thymus gland should weigh several times the expected weight for the body mass (3)It should represent more than 2% of the body mass. Diagnosis of an enlarged thymus on a chest radiograph may be problematic as its size, shape, position and growth pattern are variable1. Other anterior mediastinal masses that present in children are: teratomas, lymphosarcoma, lymphangioma, hemangioma, substernal thyroid, thymic tumor and thymolipomas and must be considered in differential diagnosis. CT scan is helpful in differentiating the thymic lesion from others4. The management of large thymic mass is controversial. When the mass is asymptomatic and the patient is less than two years of age, the patient can be followed under close observation, the mass often regresses with or without steroid administration5. Thymolytic effects of steroids are well documented, but this test is inconsistent and lacks specificity2,3. in children under 2 years of age, asymptomatic mass can be observed and a trial of steroid given, as in this age group lymphoma is not a major diagnostic consideration4. Follow up is required until thymus involutes. In thymic hyperplasia refractory to steroid therapy, FNA biopsy should be done. Thymic mass causing airway obstruction or affecting normal pulmonary development should be excised2,4,6.
References
1.Dimitrious G, Greenough A, Rafferty G. et al. Respiratory Distress in a neonate with an enlarged thymus. Eur, J. Pediatr.. 2000:159:237-8.
2.Lee TM. Kohl MT. Omar A. Hyperplasia of thymic gland. Singapore Med, J., 1996:37:288-90.
3.Henry E. Rice A. Alan W, Flake W. Hon T, et al. Massive thymic hyperplasia: characterization of a rare unediastinal mass. J. Peduatr. Surg.. 1994:29:1561-4
4.Parker LA. Gaisie 0. Scatliff JH Computerized and ultrasonographic findings in massive thymic hyperplasia. Clin. Pediatr.. 1985:24: 90-4.
5.Altar Z, Muraji T, Matsumoto Y, et al. Malignant mesenchymoma of the mediastunum presented as benign hyperplasia. Pediatr. Surgical. lnt., 1988:4:56-8.
6.Malone PS. Fitzgerald RJ. Aberrant thymus: a misleading meduastinal mass. J. Pediatr. Surg 1987:22.130-1.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: