
I. Masroor ( Radiology Department, Aga Khan University Hospital, Karachi. )
R. Hashmi ( Radiology Department, Aga Khan University Hospital, Karachi. )
November 2002, Volume 52, Issue 11
Case Reports
A 66 years old female presented with complaint of pain in right knee for 2 months. The laboratory findings were unremarkable. Plain radiograph of right knee showed normal bone density with reduction in joint space at femorotibial joint especially in medial compartment and patellofemoral compartment with slight varus angulation. There was marginal sclerosis and moderate degree of osteophyte formation at articular margins. A few rounded calcified loose bodies were also seen in the joint anteriorly as well as posteriorly with small amount of joint effusion (Figures 1 and 2).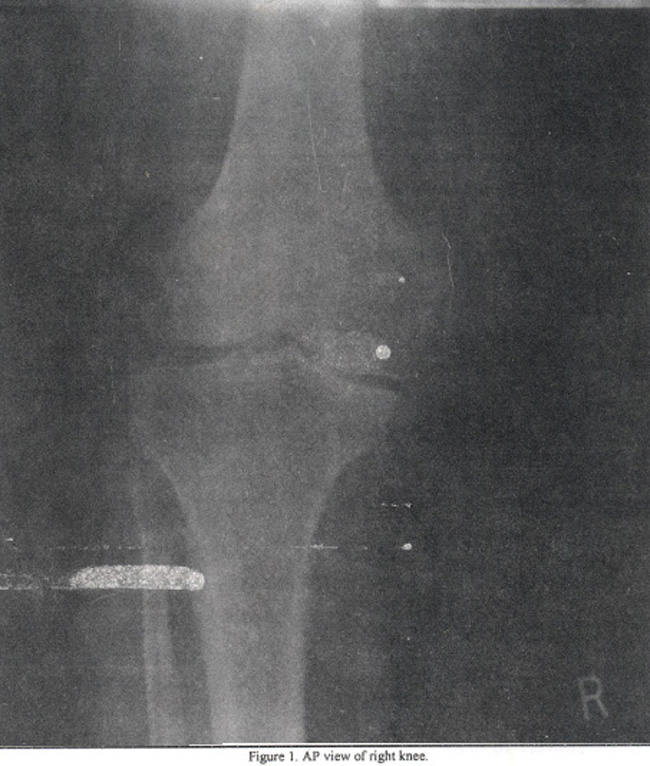

Diagnosis: Synovial osteochondromatosis with osteoarthrosis.
Discussion
Synovial osteochondromatosis is a relatively uncommon, indolent and chronic abnormality of the synovium1,2. It represents chondroid metaplasia of the synovium resulting in cartilaginous masses within a joint, bursa or tendon sheath. It is nearly always monoarticular. The knee is the site of predilection although other major joints may also be involved. It is twice as common in man as in woman and usually occurs in 3rd and 5th decade of life. Patients tend to present with a several year history of joint pain and limited range of movements.
On conventional radiographs typically there are multiple juxtaarticular rounded opacities of uniform size in and around the joint with synovial thickening and effusion1,2. In the late stages, there is erosion of adjacent bone with widening of the joint space and osteoarthritis. When multiple calcified nodules or loose bodies are present, their appearance on plain film is virtually diagnostic. On computed tomography a soft tissue mass of water density with multiple calcification is seen3. MRI appearance varies and depends upon the presence and extent of calcification and/or ossification4. CT and MRI are useful to document intra-articular location, cartilage or bone erosion, and capsular constriction or adhesive capsulitis.
On radiographs synovial osteochondromatosis could be confused with posttraumatic degeneration and calcified and ossified loose bodies1. These loose bodies tend to be larger and vary in size, in contrast to the uniform dimension of the opacities of synovial osteochondromatosis. In addition evidence of old fracture is often present. Differential diagnosis includes other pathologies causing periarticular soft tissue calcifications e.g. pigmented villonodular synovitis, synovial hemangioma, rheumatoid arthritis and tuberculosis5.
References
1.Peh WC. Synovial osteochondromatosis. Am. J. Orthop., 2001; 30:165.
2.Crotty JM, Monu JU, Pope TL Jr. Synovial osteochondromatosis. Radio!. Clin. North Am., 1996;34: 327-42.
3.Hermann G, Abdelwahab IF, Klein M, et al. Synovial chondromatosis. Skeletal Radiology, 1995;24: 298-300.
4.Ginaldi S. Computed tomography feature of synovial osteochondromatosis. Skeletal Radiol.,1980;5: 219-22.
5.Blandino A, Salvi L, Chirico G, et al. Synovial osteochondromatosis of the ankle: MR findings. Clin. Imaging, 1992;16:34-36.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: