
Mosharraf Hossain ( Respiratory Wing, Department of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. )
Abul Kalam Azzad ( Respiratory Wing, Department of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. )
Samprity Islam ( Respiratory Wing, Department of Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. )
Mohibul Aziz ( Department of Surgery, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh. )
July 2010, Volume 60, Issue 7
Case Reports
Abstract
Tuberculosis (TB) usually involves the lungs and hilar lymph nodes. Musculoskeletal TB occurs in 1%-3% of patients with TB, while chest wall TB constitutes 1%-5% of all cases of musculoskeletal TB. The present case reports a twenty six year old immunocompetent patient with multiple chest wall tuberculous abscesses along with multiple ribs destruction, in absence of active pulmonary TB or intrathoracic lymphadenopathy. Chest wall TB though rare, should have a high degree of suspicion in multiple destructive bone lesions, especially in patients from regions where TB is endemic. Plain chest x-ray postero-anterior (CXR-PA) view revealed osteolytic rib lesions with overlying opacities; fine needle aspiration cytology (FNAC) was not helpful. Computerized tomography (CT) of thorax and histopathology of the biopsied unhealthy tissue from the cavity were consistent with the diagnosis of TB. Oral anti-tubercular therapy (ATT) was given for 12 months, following which the chest wall abscesses and rib lesions healed.
Introduction
Chest wall Tuberculosis (TB) constitutes 1% to 5% of all cases of musculoskeletal TB which represents 1% to 2% of TB overall.1,2 TB is considered second only to metastasis as a cause of rib destruction3 and is thought to be the most commonly encountered inflammatory lesion of the ribs.4 Chest wall TB diagnosis is usually delayed by several weeks due to a lack of awareness and an absence of specific sign and symptoms,5 a high degree of suspicion in multiple destructive bone lesions prompt diagnosis.6 This case report presents a case of chest wall TB in a twenty six year old immunocompetent patient with multiple chest wall abscesses and ribs destruction, in the absence of active pulmonary TB or evidence of intrathoracic lymphadenopathy. With the resurgence of TB all over the world, this case report may assist in the management of chest wall TB.
Case Report
A 26 year old Bangladeshi male was admitted in the Respiratory wing, Bangabandhu Sheikh Mujib Medical University Hospital, Dhaka in June, 2007 with the complaints of multiple painful swelling in the chest. He was well 5 months ago, since then he developed swellings in the left upper chest and lower part of right chest. The swellings were painful and gradually increasing in size. He also complained of weight loss of 6 killograms (Kg), but no fever, cough or breathlessness. He was vaccinated for TB. Also, he was never diagnosed as a case of TB or had no contact with a tuberculous patient in the past. By occupation he was a garments worker and lived in a crowded slum area. On admission (May 25, 2007), he was afebrile, his pulse was 76 per minute, blood pressure was 100/60 mm Hg and body weight (BW) was 44 kg. Chest examination revealed soft, tender swelling, sized 8.5×9.5 cm2 and 6.5×7.5cm2, on the left 2nd and 3rd intercostal spaces (ICS) along mid clavicular line (MCL) and right 6th and 7th ICS along mid axillary line (MAL) respectively; local temperature was normal and there was no discharging sinus or tract. The breath sound was vesicular, with pleural rub near right chest swelling. There was no lymphadenopathy or organomegaly.
Laboratory test showed that complete blood count (CBC) was normal with haemoglobin (Hb) 13.3 gm/dl and erythrocyte sedimentation rate (ESR) 25 mm in 1st hour. Mantoux test (MT) was 17mm after 48 hours. CXR-PA was done on 07/06/07 showed ribs destruction in the right 6th rib with overlying dense opacity having convex inner margin and left 2nd rib associated with over lying dense opacity (Figure-1a).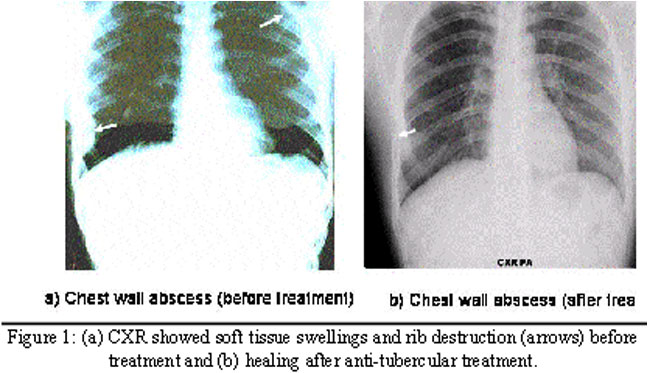
Computerised tomography (CT) scan done on 28/06/07 showed lytic lesions in anterior part of left 2nd rib (Figure-2a) and antero-lateral aspect of the right 6th rib with associated enhancing lesion having both intra- and extra-thoracic components suggestive of chest wall abscesses; no parenchymal lesion or mediastinal lympadenopathy was noted. FNAC of anterior chest wall swelling showed scanty inflammatory cells in thin fluid; acid fact bacilli (AFB) stain, gram stain and culture for AFB were negative. Incision and drainage of anterior chest wall swelling was done; about 10 ml of turbid, serous fluid poured out of the abscess, the soft tissues were then debrided and specimens were sent for histological and microbiological analysis. The tissue fragments submitted for histologic examination consisted of fibroconnective tissue with necrotizing granulomatous inflammation. There were large areas of necrosis, which were lined by epithelioid histiocytes, Langhans type giant cells and fibroblasts conclusive for TB. AFB smears and culture was negative.
On the basis of clinical features, compatible CT of thorax and histopathology report, ATT was started on 01/07/07 including Rifampicin, Isoniazid, Ethambutal, and Pyrazinamide and continued for 2 months; then Rifampicin and Isoniazid for next 10 months. Tab prednisolone 40 mg was added with ATT for 2 weeks, then it was tapered in next 4 weeks when the size of the chest wall swellings slightly enlarged after few days of starting ATT. Aspiration with a 18 gauge needle was done twice during along with ATT; almost 8 cc serosanguinous aspirate was taken out from anterior swelling. The chest wall swellings gradually diminished in size, patient gained 6 kg weight; however, chest wall was slightly depressed along right MCL.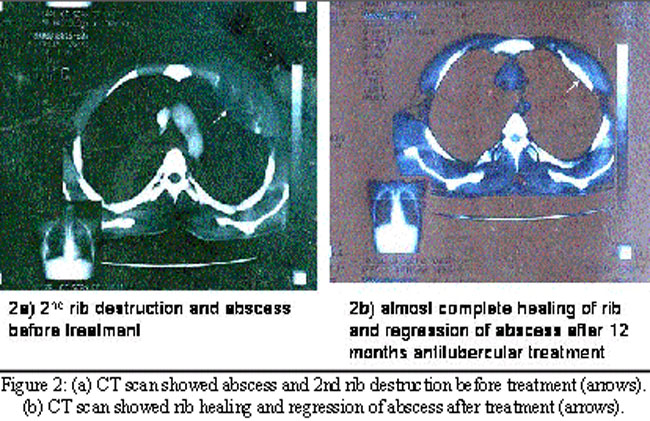
The CXR-PA (Figure-1b) of 6 months later revealed almost complete healing of both ribs and disappearance of dense opacities. CT of 12/04/08 (Figure-2b) showed healing of both ribs and complete regression of left and partial regression of right soft tissue swellings. ATT was continued till June 30, 2008. A follow up after one year later,showed no evidence of relapse.
Discussion
TB has been a major cause of morbidity and mortality, especially in the developing parts of the world. Chest wall TB is common in young adult and usually presents with chest wall swelling and/or discharging sinus, as was in our case.7,8 Bone TB is thought to result from either lymphatic or haematogenous dissemination of bacilli from a site of primary infection a Ghon\'s focus, in the lungs. The rib affection on the basis of histopathological study is mostly due to a lymph-borne dissemination of tubercle bacilli. The history of tubercular infection in the past is helpful to suggest the possibility of rib TB, though it is not always present, as was in our case.9 Tuberculous abscesses of the chest wall can involve the sternum, costochondral junctions, rib shafts, cost vertebral joints and the vertebrae. They are most frequently found at the margins of the sternum and rib shaft is the commonest location (60%),9 as was evident in our case.
Laboratory investigations like Complete blod picture (CBC), erythrocyte sedimentation rate (ESR), C - reactive protein (CRP) are usually unremarkable,10 as was evident in our case. CXR-PA view showed osteolytic lesions with overlying dense opacities, but it was not consistent with TB rather revealed the possibilities of malignancies, such as Ewing sarcoma, fibro-sarcoma, multiple myeloma and secondaries from liver, breast, thyroid and kidney.4 CT scan of chest wall TB typically manifests as osseous and cartilaginous destruction and soft-tissue masses with calcification and rim enhancement following intravenous administration of contrast material,2 which was evident in our case except calcification and rim enhancement. FNAC is not a helpful diagnostic tool for TB,9 as was in our case but FNAC excludes soft tissue extension of a neoplastic process, thus limiting the diagnostic considerations.8 Histopathology of the biopsied tissue from the cavity wall is conclusive for TB,7,8 as it was in our case. To establish microbiological proof of TB, AFB smear, AFB culture of the biopsied tissue may be negative,8 as was in our case. When, available polymerase chain reaction (PCR) is helpful,8 which was not performed in our case. Chest wall TB diagnosis is delayed by several weeks,5 as it was in our case, where it was 24 hours. In majority of the studies, the treatment of chest wall TB needs wide debridement of the abscess wall, as was done in our case and resection of diseased rib (if needed), along with ATT for 12 months.7,8,10
Conclusion
Chest wall TB though rare, should be considered even in an immunocompetent patient, in areas of high endemicity for TB or an immigrant from endemic area. CT of thorax and an excision biopsy in the diagnostic process facilitates prompt diagnosis and the effective management, to prevent bone and joint destruction.
References
1.Yao DC, Sartoris DJ. Musculoskeletal tuberculosis. Radiol Clin North Am 1995; 33: 679-89.
2.Morris BS, Maheshwari M, Chalwa A. Chest wall tuberculosis: A review of CT appearances. Br J Radiol 2004; 77: 449-57.
3.Tatelman M, Drouillard EJP. Tuberculosis of the ribs. Am J Roentgenol Radium Ther Nucl Med 1953; 70: 923-35.
4.Wolstein D, Rabinowitz JG, Twersky J. Tuberculosis of the rib. J Can Assoc Radio 1974; 25: 307-9.
5.Newton P, Sharp J, Barnes KL. Bone and joint tuberculosis in greater Manchester 1969-1979. Ann Rheum Dis 1982; 41: 1-6.
6.Chang DS, Rafii M, McGuinness G, Jagirdar JS. Primary multifocal tuberculous osteomyelitis with involvement of the ribs. Skeletal Radiol 1998; 27: 641-5.
7.Agrawal V, Joshi MK, Jain BK, Mohanty D, Gupta A. Tuberculotic osteomyelitis of rib--a surgical entity. Interact Cardiovasc Thorac Surg 2008; 7: 1028-30.
8.Mohanty D, Agrawal V, Jain BK, Gupta R, Rathi V, Gupta A. Osteomyelitis of the ribs: a strategy for prompt diagnosis and effective management, Trop Doct 2008; 38: 239-41.
9.Faure E, Souilamas R, Riquet M, Chehab A, Le Pimpec- Barthes F, Manac\'h D, et al. Cold abscess of the chest wall: a surgical entity? Ann Thorac Surg 1998; 66: 1174-9.
10.Ozol D, Köktener A, Uyar ME. Active pulmonary tuberculosis with vertebra and rib involvement: case report. South Med J 2006; 99: 171-3.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: