
Saulat Hasnain Fatimi ( Division of Cardiothoracic Surgery, Department of Surgery, The Aga Khan University Hospital, Karachi, Pakistan. )
Umair Khalid ( Class of 2009, Medical College, The Aga Khan University Hospital, Karachi, Pakistan. )
Sanna Fatima ( Class of 2009, Medical College, The Aga Khan University Hospital, Karachi, Pakistan. )
Taimur Saleem ( Class of 2009, Medical College, The Aga Khan University Hospital, Karachi, Pakistan. )
July 2010, Volume 60, Issue 7
Case Reports
Abstract
Empyema is a devastating complication that is rarely seen in the postpneumonectomy setting. A 56 years old man presented to us 24 years after pneumonectomy with a 15 days history of chest pain and shortness of breath. Physical examination revealed a fluctuant swelling at the thoracotomy site. Computed tomography scan showed a large fluid density mass in the left pneumonectomy space. Needle aspiration and video assisted thoracoscopic surgery was carried out and culture of the aspirated fluid grew Pseudomonas aeruginosa. The patient was discharged with the chest tubes in place. At 2 months follow-up, the patient presented with fever and continuous copious drainage of pus from empyema tubes. Piperacillin with tazobactam at 4.5 grams per day helped in the resolution of fever but the output from the empyema tubes continued. An open window thoracostomy was performed and the patient was discharged on standard dosage of cefixime and fusidic acid. Following this antibiotic regimen, he remained stable with complete resolution of the infection.
Introduction
Empyema can develop in a number of settings including thoracic surgeries, bronchopleural fistulas, mediastinal infections and trauma.1,2 Postpneumonectomy empyema (PPE) is a rare but formidable clinical entity that ranges in incidence from 2-15% according to published literature.3,4 We describe a case of late-onset PPE whereby the patient developed empyema 24 years following the pneumonectomy.
Case History
A 56 years old gentleman presented with the complaint of left sided chest pain since 15 days. This was associated with shortness of breath on exertion. The pain was localized to a fluctuant swelling at the thoracotomy incision site. He was afebrile at the time of presentation and had no prior history of fever. His past surgical history was remarkable for a left sided pneumonectomy 24 years ago because of intractable haemoptysis secondary to pulmonary tuberculosis. The remaining history was unremarkable. On physical examination, the absence of breath sounds was consistent with the surgical history of left sided pneumonectomy.
A chest roentogram revealed compensatory hyperinflation of the right lung. Computed tomography (CT) scan showed large fluid density mass in left posterior pneumonectomy space (Figure-1).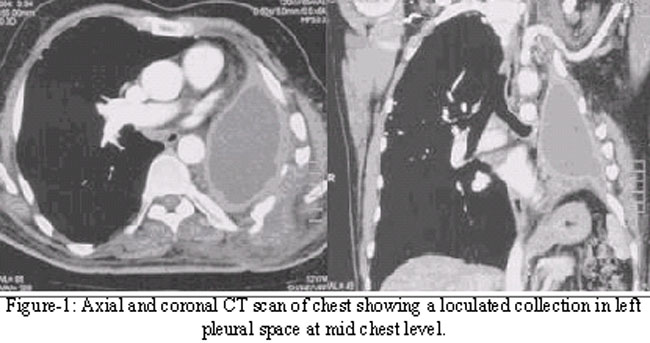
This loculated fluid collection in the left pleural cavity measured 10 cm x 5 cm (cranio-caudal and transverse). Flexible bronchoscopy was performed, which showed no evidence of bronchial leak or inflammation.
Using needle aspiration technique, 100cm3 of thick pus was drained out of the pleural cavity. Video thoracoscope was then introduced into the chest cavity and subsequently 200 cm3 of thick pus was drained from the pleural cavity. Thick fibrosis was noted in the entire left lung space. Multiple biopsies were taken, pleural cavity was thoroughly irrigated with saline and empyema tubes were placed.
The culture of the aspirated fluid grew Pseudomonas aeruginosa. Histopathology examination of the biopsy samples revealed non-specific acute-on-chronic inflammation along with foreign body type giant cells. There was no evidence of malignancy. Fungal cultures and acid fast bacillus smear and culture were all negative. The patient\'s hospital stay was unremarkable and he was discharged after two days with empyema tubes in place.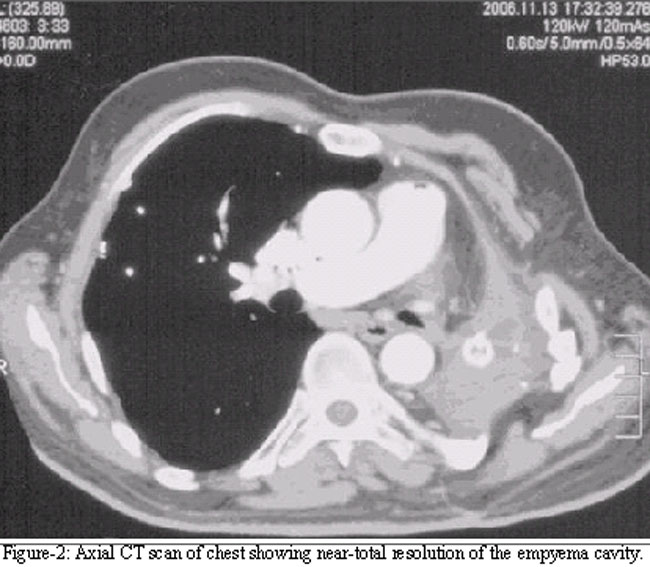
Figure-2 shows post video assisted thoracoscopic surgery (VATS) CT scan with resolving empyema cavity.
However, at 2 months follow-up the patient presented with high grade fever and continuous copious drainage of about 100cm3/day of pus fluid from the empyema tubes. Culture of the draining fluid again grew P. aeruginosa colonies. He was started on piperacillin with tazobactam at a dosage of 4.5g/day for 6 weeks. He consequently became afebrile and the output from the tubes reduced to about 35 cm3/day. Over the next six months he remained afebrile, although the discharge from the empyema tubes continued.
An open window thoracotomy was performed next and the patient was discharged on a regimen of cefixime and fusidic acid for 6 weeks. Following this antibiotic regimen, he remained stable with complete resolution of the infection and had no issues at one year follow up.
Discussion
Rudolph Nissen carried out the first successful pneumonectomy in 1931. Since then empyema and bronchopleural fistula (BPF) have continued to be devastating complications after pneumonectomy.1 The overall perioperative mortality rate of pneumonectomy is less than 7%. However, this figure escalates to 25% when complicated by an empyema and to 50% when complicated by BPF.2 The incidence of empyema has been reported to increase when there is a concomitant BPF.2
A number of organisms are responsible for causing empyema, the most common ones being Streptococcus pneumoniae, Staphylococcus aureus, and group A streptococci. However, it should also be noted that as many as 20% of the cases turn out to be sterile, even after the drained frank pus is cultured. This is largely attributed to the widespread use of antibiotics before drainage procedures.2
Our patient presented with a fluctuant swelling at the site of the previous thoracotomy incision. However, late-onset PPE presents with vague symptoms and minimal signs in most cases. Physical examination of the respiratory system becomes fallacious in the absence of lung architecture on the affected side in the setting of a previous pneumonectomy. Non-specific symptoms in patients with late onset PPE include anorexia, temperature elevation, weight loss, chest discomfort, and pain.5 When a patient with a past surgical history of pneumonectomy presents with signs and symptoms of infection, the pneumonectomy space must be vigilantly investigated and evaluated as a possible site for infection. The duration of time that may have lapsed from the operation should not lull the clinician into a fall sense of security and a high index of suspicion must be maintained to prevent the delay in the diagnosis of this entity.
The cause of late-onset PPE in the majority of cases is the haematogenous spread of bacteria. After pneumonectomy, fluid that accumulates in the pleural space clots and becomes fibrotic. However, the space is not completely obliterated. Small areas of fluid remain even years after the pneumonectomy and they can serve as potential sites for bacterial seeding.5 It is important to rule out any leaks from the bronchial tree in patients with PPE. Although the cornerstones of management remain the same, additional surgical techniques are warranted if such leaks are discovered. We evaluated our patient for bronchial pathology using flexible bronchoscopy.
Dogmatic consensus on the most optimum modus operandi for the management of late onset PPE remains elusive. A number of management strategies have been described in literature with varying success rates. Fenestration was first developed by Eloesser in 1935 as a technique for managing tuberculous empyemas. This approach was later adapted by Clagett and Geraci in 1963 for the treatment of PPE.6 Earlier case studies with the use of fenestration showed a better treatment profile as compared to irrigation and tube thoracostomy. However, irrigation and tube thoracotomy was slightly better than fenestration on analysis of outcomes of second intervention.6
In a case series,8 cases were reported in which PPE developed at least 3 months after pneumonectomy. Treatment involved rib resection and open drainage without tubes.4 Another case study reported a patient who developed empyema 13 years after pneumonectomy and who was successfully treated using an omental pedicle flap. 88 In another report, a man presenting with empyema 38 years after pneumonectomy was treated with open-window thoracostomy.9
The treatment of PPE has run across a gamut of approaches and techniques over the years. Although simpler and minimally invasive procedures such as VATS should suffice in most patients, PPE can be difficult to treat occasionally. Open window thoracostomy or other interventions such as myoplasty or thoracoplasty may need to be opted for in such circumstances. 10 The need for regular follow up in patients with PPE cannot be overemphasized; although consensus on the regularity and number of follow ups is needed. Follow-ups are important to document complete resolution of the empyema and they also provide a timely opportunity to evaluate the need for additional intervention strategies such as open window thoracotomy. VATS in conjunction with needle aspiration should be explored further in future studies to evaluate safety and efficacy.
Conclusion
We have presented an unusual case whereby a patient developed empyema 24 years after pneumonectomy. Regular follow-ups provided an opportunity for additional intervention in this patient; ultimately culminating in the complete resolution of an otherwise resilient infection.
References
1.Deschamps C, Bernard A, Nichols FC 3rd, Allen MS, Miller DL, Trastek VF, et al. Empyema and bronchopleural fistula after pneumonectomy: factors affecting incidence. Ann Thorac Surg 2001; 72: 243-8.
2.Goldstraw P. Postpneumonectomy empyema. J R Soc Med 1993; 86: 559-60.
3.Deschamps C, Pairolero P, Allen M, Trastek V. Management of postpneumonectomy empyema and bronchopleural fistula. Chest Surg Clin N Am 1996; 6: 519-27.
4.Zaheer S, Allen MS, Cassivi SD, Nichols FC 3rd, Johnson CH, Deschamps C, et al. Postpneumonectomy Empyema: Results After the Clagett Procedure. Ann Thorac Surg 2006; 82: 279-87.
5.Gossot D, Stern JB, Galetta D, Debrosse D, Girard P, Caliandro R, et al. Thoracoscopic management of postpneumonectomy empyema. Ann Thorac Surg 2004; 78: 273-6.
6.Goldstraw P. Treatment of postpneumonectomy empyema: the case for fenestration. Thorax 1979; 34: 740-5.
7.Kerr WF. Late-onset post-pneumonectomy empyema. Thorax 1977; 32: 149-54.
8.Tsubota N, Hatta T, Yoshimura M, Yanagawa M. A case of empyema developing thirteen years after a pneumonectomy treated using pedicled omentum which was followed by intestinal obstruction. Jpn J Surg 1991; 21: 703-5.
9.Alifano M, Magdeleinat P, Regnard JF. Unusual imaging of late postpneumonectomy empyema. Ann Thorac Surg 2002; 74: 935.
10.Van Raemdonck D, Kesteman J, Roekaerts F, Jadoul P. Treatment of postpneumonectomy empyema with or without bronchopleural fistula. Acta Chir Belg 1990; 90: 59-66.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: