
Humera Ahsan ( Department of Radiology, Aga Khan University Hospital, Karachi, Pakistan. )
Muhammad Akbar ( Department of Radiology, Aga Khan University Hospital, Karachi, Pakistan. )
Atta-ul-Aleem Bhatti ( Department of Neurosurgery, Aga Khan University Hospital, Karachi, Pakistan. )
November 2009, Volume 59, Issue 11
Case Series
Abstract
The objective of the study was to introduce the availability of bold imaging facility at Aga Khan University Hospital Karachi for the first time in Pakistan and also to review the practical application and advantages of functional magnetic resonance imaging (fMRI) and blood oxygen level dependant (BOLD) Imaging Procedures. The study was conducted at Aga Khan University Hospital, Karachi from August 2008 to November 2008 .Three patients were selected that had presented with intracranial space occupying lesions. They underwent Functional Magnetic Resonance Imaging (fMRI). The findings of the images were important to describe and localize the eloquent brain areas and their relationship to the underlying pathology. In conclusion this study reflected the significance of the Blood Oxygen Level Dependant (BOLD) imaging modality that can help in improved outcome of patients presenting with intracranial space occupying lesions.
Introduction
The Magnetic Resonance Imaging (MRI) of human brain has well recognized importance in relation to detail elaboration. In 1991, contrast bolus tracking technique was described by Belluveau of the Massachusetts General Hospital who established a connection between MRI and cortical function. This was demonstrated by means of a paramagnetic contrast that was administered as a bolus. The activity noted was a signal change due to accumulation of that contrast, due to increased blood flow to the occipital cortex after photo-stimulation.1 In 1992, Dr. Seiji Ogawa described a modified functional Magnetic resonance imaging (fMRI) technique that utilized only deoxyhaemoglobin and required no administration of any external contrast agent. According to him, neurons involved in increased brain activity require increased blood flow and subsequent increase oxygen requirement. It is the presence of deoxyhaemoglobin, an endogenous contrast agent, in hyper functioning brain areas that results in development of magnetic signal variation as detected on the MRI scanner.2
The fMRI study requires subjects to carry out various tasks depending on the cortical area in consideration. The subject may be to press buttons, tap the fingers, asked to imagine something, shown a movie or made to hear sounds or smell odours. Only those tasks are allowed that do not involve any head movement due to increased sensitivity of the study. Time varies from fifteen minutes to two hours. T1 weighted Images are acquired which are later superimposed upon the T2 images, using the Blood Oxygen Level Dependant (BOLD) technique. After computer analysis images are finally developed for interpretation.
The advantages of fMRI are following:
(1) Non-invasive.3
(2) Comparatively cheap, as no tracer or contrast required.4
(3) Correlated to predicting recovery after a neurological event.4
(4) Pre and post operative comparison in term of anatomical and physiological function.5
The disadvantages of fMRI are as follows:
(1) Imaging procedure may capture unwanted artifacts.
(2) It is an indirect measure of brain activity that may be influenced by non-neural changes in the body.
This case series is presented to assess the BOLD images in patients diagnosed with intracranial space occupying lesions.
Method
A case series study was conducted from August to November 2008, including patients that were previously diagnosed with intracranial space occupying lesion at Aga Khan University Hospital and underwent MRI with additional BOLD imaging. All the imaging procedures were done on SIEMENS model MAGNETOM AVANTO 1.5tesla Tim technology (76x18) SQ-engine. To assess the motor cortex the BOLD images were acquired after "Finger Tapping" in each patient. The following is a brief description of the cases along with the relevant observations.
Case 1:
A 23-year-old right handed male presented with history of generalized tonic clonic seizures over a duration of four months. His plain MRI scan revealed a left sided frontal lobe lesion which was hyperintense on T2 and ISO to hypointense on T1 weighted images. Additional magnetic resonance spectroscopy with attention to the involved area, suggested a malignant lesion on basis of increased choline peak and low N-acetylaspartate (NAA). Pre-operative fMRI defined the motor cortices and their sparing at a distance of 3 cm from the mass on axial section. The patient underwent craniotomy with excision of the left frontal space occupying lesion. The mass was identified to be an anaplastic oligodendroglioma grade III on Histopathology. Post-operatively, the patient recovered successfully.
Case 2:
This was a 34-year-old right handed man presenting with headaches and dizziness for past 7 months. His plain MRI revealed a large left sided parietal mass that was located medially towards the midline. fMRI study demonstrated the motor cortex lying above and unharmed from the mass at a distance of 3-4 cm but the patient was lost to follow up subsequently.
Case 3:
This was a 45-year-old leukaemic patient who presented with the complaints of intermittent headaches associated with vomiting and visual blurring for the past one month. Magnetic resonance imaging demonstrated an abnormal signal intensity mass in left parieto-occipital region measuring 5.2x3.3x2.8 cm. in size and with associated mass effect towards left side of mid-brain. This was hyperintense on T2 and hypointense on T1 weighted images. fMRI demonstrated sparing of the left motor cortex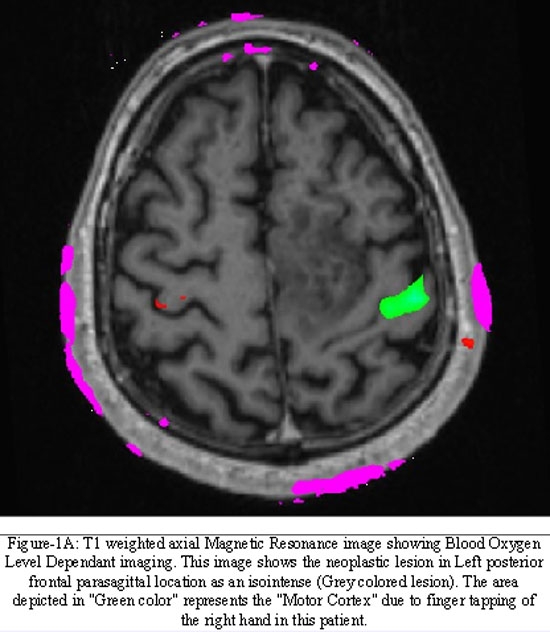
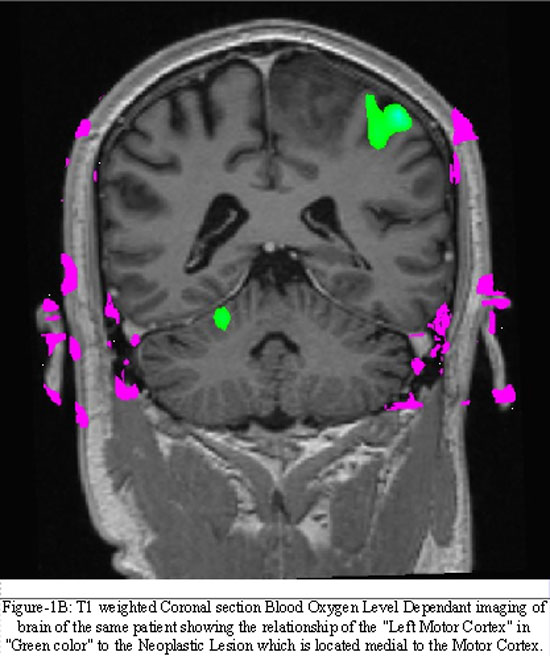
by a distance of 1 cm. He underwent trans-cranial biopsy for the brain lesion that revealed astrocytoma grade III on histopathology. The patient is currently under chemotherapy (Figure 1A & 1B).
Discussion
Various studies have verified that fMRI for pre surgical planning, can positively affect a patient's surgical outcome. This technique helps, neurosurgeons by providing additional knowledge regarding the functional area surrounding as space occupying lesion thereby increasing surgical confidence and allowing surgeons to be more aggressive with their surgical plan, increasing the likelihood for a successful resection. As evident by a research conducted between one group undergoing fMRI and consequent surgery to another group undergoing conventional surgery, there was reduction in post operative neurological compromise for the former.6
There is also evidence relating signal changes in BOLD imaging of patients recovering from stroke event as compared to normal controls. It seems that there is cerebral disorganization after recovery from stroke events leading to reduced haemodynamic response with the consequent impaired Functional and BOLD image.7
Apart from cerebrovascular events there is also research being done for establishing the relation between neurodegenerative disorders and their presentation on fMRI in comparison to normal patterns. Diseases like Parkinson's show increase in brain activity in certain areas on functional imaging compared to normal person because this relative increase compensates for the lost activity in affected areas targeted by the disease.8 There is also similar loss of functional activity noted in patients with Alzheimer's disease which is greater in comparison to effects caused by aging alone.9
Additionally, there is also work in development on using fMRI to establish successful interactions between a drug and its site of effect in the CNS through the development of characteristic brain signatures as picked up on imaging. This is termed as the pharmacological fMRI. It is also predicted that such examinations will exceed the boundary of CNS to also include the spinal cord and various genetic polymorphisms that could result in different responses of drugs on the brain.10
Being a new emerging and revolutionary technique, fMRI will soon be included as a protocol for patient management.
References
1.Belliveau JW, Kennedy DNF, McKinstry RC, Buchbinder BR, Weisskoff RM, Cohen MS, et al. Functional mapping of the human visual cortex by magnetic resonance imaging. Science 1991; 254: 716-9.
2.Ogawa S, Tank DW, Menon R, Ellermann JM, Merkle H, Ugurbil K. Proceedings of National Academy of Sciences of the United States of America. Proc Natl Acad Sci 1992; 89: 5951-5.
3.Baudelet C, Gallez B. Current Issues in the Utility of Blood Oxygen Level Dependent MRI for the Assessment of Modulations in Tumor Oxygenation Current Medical Imaging Reviews 2005; 1: 229-43.
4.Ogawa S, Lee TM, Kay AR, Tank DW. Brain magnetic resonance imaging with contrast dependent on blood oxygenation . Proc Natt Acad Sci USA 1990; 87: 9868-72.
5.Holodny AI, Schulder M, Liu WC, Maldjian JA, Kalnin AJ. Decreased BOLD Functional MR Activation of the Motor and Sensory Cortices adjacent to a Glioblastoma Multiforme: Implications for Image-Guided Neurosurgery. Am J Neuroradiol 1999; 20: 609-12.
6.Winkler D, Lindner D, Trantakis C, Strauss G, Richter A, Georgiadis MH, et al. The Importance of Functional Magnetic Resonance Imaging in Neurosurgical Treatment of Tumors in the Central Region. Clinical Neuroradiology 2005; 15: 182-9.
7.Krainik A, Georgiadis MH, Zysset S, von Cramon Y. Regional impairment of cerebrovascular reactivity and BOLD signal in adults after stroke. Stroke 2005; 36: 1146-52.
8.Wu T, Hallett M. A functional Magnetic Resonance Image study of automatic movements in patients with Parkinson's disease. BRAIN 2005; 28: 2250-9.
9.Murphy C, Ducastel BC, Haney RC, Gilbert PE, Ferdon S. ERP, fMRI and Functional Connectivity Studies of Brain Response to Odor in Normal Aging and Alzheimer's disease. Chemical Senses 2005; 30: 170-1.
10.Borsook D, Becerra L, Hargreaves R. A role for fMRI in optimizing CNS drug development. Nature reviews Drug discovery 2006; 5: 411-24.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: