
Ayesha Khan ( Al-Shifa Trust Eye Hospital, Jhelum Road, Rawalpindi, Pakistan. )
Saemah Nuzhat Zafar ( Al-Shifa Trust Eye Hospital, Jhelum Road, Rawalpindi, Pakistan. )
November 2009, Volume 59, Issue 11
Case Series
Abstract
Nanophthalmos is an uncommon developmental ocular disorder characterized by a small eye with short axial length, high hyperopia and high lens/eye volume ratio due to arrested development of the globe in all directions. Different types of fundus changes can rarely occur with nanophthalmos. We describe five cases of nanophthalmos, each of them presenting with a different fundus appearance. Our case series highlights variability of pigmentary changes from retinal flecks to bone spicules and bull's eye maculopathy, which are rare in the combinations described here.
Introduction
Nanophthalmos is a rare, bilateral disorder consequent upon the arrest of development of the globe in all dimensions.1 This occurs after the foetal fissure has closed and without other major malformations. It is characterized by short axial lengths, usually less than 20.00mm, and extreme hyperopia with refractive error usually in the range of +8.00 to +25.00 dioptres (DS). Characteristic features include normal cornea to microcornea, shallow anterior chamber and high lens/globe ratio. There is a considerably thickened choroidal vascular bed and scleral coat.2 Abnormal scleral collagen has been found to be a cause of uveal effusion in patients with nanophthalmos.3 The best corrected visual acuity is rarely better than 20/40. Patients with nanophthalmos in the present study had cycloplegic refraction, best corrected visual acuity assessments using ETDRS and Lea charts, slit-lamp and fundus examinations, intraocular pressure measurement, fundus photography and ultrasonographic examination using A-mode and B-mode. Electrodiagnostic tests were not carried out. We describe five cases of nanophthalmos, each of them presenting with a different fundus appearance.
Case-1:
A 10-year-old girl presented with fine pendular nystagmus and best corrected visual acuity (BCVA) 1/60 in both eyes (OU). She had a refractive correction of +7 / +2.5 at 90 in the right eye (OD) and + 6/ +2.5 at 90 in the left eye (OS). She had eccentric fixation in both eyes with the fixing eye in exotropia (XT). There was no history of nyctalopia or hemeralopia. She was born of consanguineous parents, had 3 siblings with history of reduced vision and her two paternal cousins were blind. Intraocular pressure (IOP) measured with applanation tonometry was 18 mm Hg in both eyes. Her horizontal corneal diameters were 11mm in both eyes. Axial length in right eye was 19.12 mm and in the left eye was 19.20 mm. The axial lengths ranged from 15.00-16.00mm and the refractive error was above +15.0 dioptres in her 3 siblings. The scleral thickness was above 2.2 mm in all the siblings. Fundus examination of our patient revealed bilateral pigmentary retinopathy with bull's eye maculopathy. These findings were absent in her three sisters who had shorter axial lengths and a higher refractive error as compared to our case.
Case-2:
A 21-year-old male presented with best corrected visual acuity of 6/60 OU with +18 DS refractive error in both eyes. There was no history of nyctalopia. He was an off spring of a consanguineous marriage. Siblings were not affected. On examination, he had a negative angle kappa with appearance of pseudo exotropia. IOP recorded with applanation tonometry was 10 mm Hg in both the eyes. Axial lengths were 15.80mm OD and 15.20mm OS. His corneal diameter was 10.5mm horizontally and 10.25mm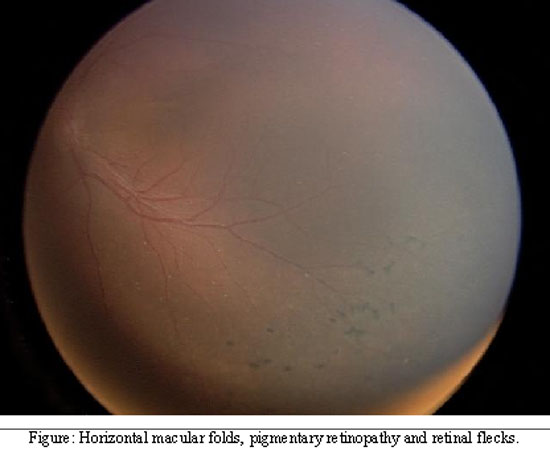
vertically OU. He had a scleral thickness of more than 3.0 mm OU. Fundus examination showed crowded discs with blurred margins along with horizontal macular folds emanating from the disc margin and extending temporally to just beyond the fovea. Peripheral fundus showed pigmentary retinopathy and retinal flecks (Figure). Optical coherence tomography (OCT) showed an elevated chorioretinal fold of normal thickness with an underlying empty vaulted area. He was advised tablet acetazolamide 250 mg x 12 hourly. His vision subsequently improved to 6/24 OU however his fundus appearance and OCT findings remained unchanged.
Case-3:
A 7-year-old boy presented with best corrected vision of 6/18 in both eyes with a correction of +15DS OU. His IOP, as measured with tonopen, was 20 mm OD and 16 mm OS. Horizontal corneal diameter was 11mm in both eyes. Axial lengths were 15.83 mm in the right eye and 15.75 mm in the left eye. Parental consanguinity was present. Siblings were not affected. Scleral thickness measured to 2.4mm OU. On fundus examination the macula had an enhanced yellow reflex in the papillomacular region and the peripheral fundus showed white dots outside the vascular arcades.
Case-4:
A 3-year-old boy presented with best corrected visual acuity of 0.5 cycles per centimeter (cpcm) OU using Lea Gratings (Snellen approximately <6/240). His IOP was 10 mm OU with tonopen. His axial lengths were of 18.06 OD and 18.15 OS. He had a refractive error of +10.00 dioptres OU. His scleral thickness measured 2.2 mm OU. He was off spring of consanguineous marriage and the siblings were not affected. On fundus examination, there were flecks on the macula in both eyes, temporal to the fovea. Peripheral fundus examination did not reveal any abnormality.
Case-5:
A 6-year-old boy had best corrected vision of 2/60 OU with refractive error of +8.00 DS. He had nystagmus with a history of hemeralopia. IOP was 15mmHg in the right and 13 mmHg in the left eye as measured with tonopen. He had small angle left exotropia. His horizontal corneal diameter was 8.5mm and vertical corneal diameter was 8mm OU. His axial lengths was 19.11mm OD and 19.19 mm OS. He had a scleral thickness of 2.3 mm OU. There was parental consanguinity and the siblings were not affected. Fundus examination revealed bull's eye maculopathy in both eyes. There were no flecks or pigmentary retinopathy.
Nanophthalmic patients described in our report have a variety of combinations of retinal findings. These include pigmentary retinopathy with bull's eye maculopathy in one patient, pigmentary retinopathy, white dots in retina and macular folds in another patient, white flecks in the retina in the macular area and outside the vascular arcades respectively in two other patients, without pigmentary retinopathy. One patient had bull's eye maculopathy in both eyes without pigmentary retinopathy. Among these variable findings on fundus examination, axial lengths were not as short in patients with features of bull's eye maculopathy (19mm), as found in the rest (average mean 16.43mm). Patients with axial lengths more than 18mm did not show crowded discs, yellowish reflex or macular folds (Table).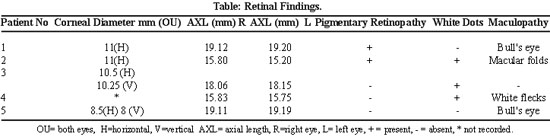
Discussion
Various macular lesions have rarely been associated with nanophthalmic eyes. Papillomacular folds and macular radial folds have been described.4,5 Foveal avascular zone abnormalities in nanophthalmic eyes has been reported.6 Pigmentary retinal degeneration also rarely occurs with nanophthalmos.7 None of our patients had nyctalopia. The macular lesions and white dots in the retina reported here also make an uncommon association. In our case series the patients with more than 18mm axial lengths did not show crowded discs, yellowish reflex or macular folds, understandably because of less crowding of the posterior segment. Early detection using ultrasound biomicroscopy of patients with high hyperopia may help in timely intervention such as refractive correction, amblyopia therapy and scleral surgery if indicated in cases with uveal effusion syndrome. We did not see uveal effusion in any patient in the present case series. Autosomal recessive (AR) form of nanophthalmos (NNO2) can be caused by mutation in the gene encoding membrane-type frizzled-related protein (MFRP). Our cases seem to have autosomal recessive pattern of inheritance of the disease. The variety of retinal findings, in the patients in our study are rare features, in the combinations described.
Conclusion
The above case series highlights the fact that nanophthalmaic patients may present with fundus findings of different types of pigmentary changes from retinal flecks to bone spicules and bull's eye maculopathy. Vision may be affected in these patients due to high refractive amblyopia and any associated chorioretinal changes.
References
1.Nischal KK. Developmental Anomalies of the Anterior Segment and Globe. In: Wright KW, Spiegel PH, editors. Pediatric Ophthalmology and Strabismus. 2nd Ed. Springer 2003; 383.
2.Spaide RF, Goldbaum M, Wong DW, Tang KC, Idia T. Serous detachment of the retina. Retina 2003; 23: 820-46.
3.Uyama M, Takahashi K, Kozaki J, Tagami N, Takada Y, Ohkuma H, et al. Uveal effusion syndrome: clinical features, surgical treatment, histologic examination of the sclera and pathophysiology. Ophthalmology 2000; 107: 441-9.
4.Serrano JC, Hodgkins PR, Taylor DS, Gole GA, Kriss A. The nanophthalmic macula. Br J Ophthalmol 1998; 82: 276-9.
5.Tay T, Smith JE, Berman Y, Ades L, Missotte I, Saglibene H, et al. Nanophthalmos in a Melanesian population. Clin Experiment Ophthalmol 2007; 35: 348-54.
6.Walsh MK, Goldberg MF. Abnormal foveal avascular zone in nanophthalmos. Am J Ophthalmol 2007; 143: 1067-8.
7.Proenca H, Castanheira-Dinis A, Monteiro-Grillo M. Bilateral nanophthalmos and pigmentary retinal dystrophy-an unusual syndrome. Graefes Arch Clin Exp Ophthalmol 2006; 244: 1203-5.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: