
Zahid Ullah ( Department of Pathology, Gomal Medical College, Dera Ismail Khan, Pakistan. )
Aamer Ali Khattak ( Department of Medical Lab Technology, University of Haripur, Pakistan. )
Sara Arif Ali ( Department of Pathology, Gomal Medical College, Dera Ismail Khan, Pakistan. )
Javaid Hussain ( Department of Pathology, Gomal Medical College, Dera Ismail Khan, Pakistan. )
Badshah Noor ( DHQ Teaching Hospital, Dera Ismail Khan, KPK, Pakistan. )
Raheela Bano ( Department of Pathology, Gomal Medical College, Dera Ismail Khan, Pakistan. )
Muhammad Amin Jan Mahsud ( Department of Pathology, Gomal Medical College, Dera Ismail Khan, Pakistan. )
December 2016, Volume 66, Issue 12
Original Article
Abstract
Objective: To assess the reliability of different red blood cell indices-based formulae in the indexes formula in differential diagnosis of beta thalassemia trait and iron deficiency anaemia.
Methods: This cross-sectional study was conducted between January and October 2015 in Dera Ismail Khan in the Khyber Pakhtunkhwa province of Pakistan. Patients of beta thalassemia trait and iron deficiency anaemia were registered irrespective of age and gender. About 5 mL of blood was taken from each patient to analyse different red cell parameters like red blood cell count, haemoglobin, mean cell volume, mean cell haemoglobin, mean cell haemoglobin concentration, and red cell distribution width. Five formulae were used to discriminate between the two conditions. These were red cell distribution width index, Shine and Lal index, Mentzer index, Srivastava index, and the Green and King index. Sensitivity, specificity, positive and negative predictive values and Youden\\\'s index of all the indices were calculated.
Results: Of the 800 patients, 230(29%) had beta thalassemia trait and 570(71%) had iron deficiency anaemia. The red cell distribution width index appeared be a reliable index in discriminating between beta thalassemia trait and iron deficiency anaemia with sensitivity and specificity of 100% and 93% respectively.
Conclusion: The red cell distribution width index was the most consistent index for differentiating between beta thalassemia trait and iron deficiency anaemia. IIt could be used as a screening index for beta thalassemia trait in areas where haemoglobin electrophoresis facility is unavailable.
Keywords: Beta-thalassemia trait, Iron deficiency anaemia, Red cell parameters, Hb electrophoresis, Red cell distribution width. (JPMA 66: 1627; 2016)
Introduction
Beta-thalassemia trait (BTT) and iron deficiency anaemia (IDA) are the most commonly encountered disorders of hypochromic and microcytic anaemia.1,2 A recent report by World Health Organisation (WHO) shows that out of 2 billion anaemia cases, 50% are IDA.3 High incidence of iron deficiency in developing and under-developed countries are associated with countless morbidities. Frequently it is mild but, if not treated, can lead to maternal haemorrhage due to uterine atony, arrhythmia, pregnancy-related complications, delayed growth in infants and children, and even mortality.Blood loss, parasitosis, iron-poor diet, malabsorption, multiparity, poor health of pregnant women and socio-economic burden are the key factors for IDA.4-6
Thalassemia, an inherited haemoglobinopathy, is characterised by impaired synthesis of normal globin peptide chains in haemoglobin (Hb). It is the most common genetic disorder, and its prevalence and severity are population-dependent with the type of thalassemia seen dependent on racial background. About 5% of the world\\\'s population has Hb production defects and 7% of carrier for Hb disorders. 7 Annually 0.3-0.5 million children are born with severe haemoglobinopathies; 80% of these children are from developing and underdeveloped countries.7
About 2-18% of Eastern Mediterranean population, 0-11% Southeast Asian and 0-12% in Sub-Saharan Africa harbour the thalassemia gene.8 Earlier, it was thought that North America and Northern Europe were non-endemic regions for thalassemia, but now these regions also have high incidence of thalassemia due to immigration of people from thalassemia-endemic regions.9,10
Thalassemia is a major global health problem;10% is contributed by the Middle East, 9% by Southeast Asia, and 8% from the Mediterranean region.11 Each year 5000 cases of homozygote thalassemia patients are born in Pakistan, making it one of the most prevalent inherited disorders of the country11 and about 5% of Pakistanis carry the heterozygous beta thalassemia gene.12
Definite diagnostic parameters for BTT and IDA are serum iron, ferritin and haemoglobin alpha 2 (HbA2) electrophoresis.13 Gold standards for measurement of HbA2 level for the BTT diagnosis are cellulose acetate or gel-electrophoresis and high-performance liquid chromatography techniques. 14-16
Different red cell indices provided by electronic haematological cell counter can be used to discriminate BTT and from IDA. The purpose of using indices is to reduce unnecessary investigation cost on discriminating BTT from IDA. Various red cell indices have been proposed in the past as easy and economical tools to discriminate BTT or IDA.17-21 Using red cell indices or parameters like mean cell volume (MCV), mean cell Hb (MCH), mean cell Hb concentration (MCHC) and red cell distribution width (RDW), one can differentiate BTT from IDA. Best discrimination index which has high specificity and sensitivity is the one which can detect the maximum number of BTT patients (high sensitivity) while taking out patients with IDA (high specificity). The current study was conducted to check the ability of 5 different indices-based formulae by calculating their sensitivity and specificity.
Material and Methods
This cross- sectional study was conducted between January and October 2015 in Dera Ismail Khan, a city situated on the west bank of the Indus River in Khyber Pakhtunkhwa province of Pakistan. After approval from the ethics committee of Gomal Medical College (GMC) and Hayat Medical Lab, and after taking proper informed consent from all patients/parents, blood samples were collected.
The study population comprised microcytic hypochromic anaemia patients referred for Hb electrophoresis to the GMC pathology lab. Patients included were aged 2-35 years of either gender with HB ranging from 8 g/dl to 11.5 g/dl. Patients having recent blood transfusion in the preceding four weeks and those who were critically ill were excluded. By using aseptic venepuncture blood collection, about 5mL of blood was collected and divided into Ethylenediaminetetraacetic acid (EDTA) and plain gel tube for biochemical and haematological analysis. Serum was collected from plain gel tube after centrifugation at 3000 RPM for 5 minutes for serum iron which was analysed by using Merck kits on Rayto (RT-9200) chemistry analyser.
Using an automated haematology analyser (Nihon Kohden, Tokyo), complete blood parameters, including Hb, red blood cell (RBC) count and RBC indices, like MCV, MCHC, MCH, packed cell volume (PCV) and RDW, were performed. For estimation of HbA2 level of BTT, alkaline cellulose acetate electrophoresis method (Wealtech, USA) was used.
SPSS 19 was used for statistical analysis. For screening performance of various indices for BTT, receiver operating characteristic (ROC) curve was used. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated using previously suggested formulae.22,23
Results
The five discrimination indices used in the evaluation were calculated and summarised (Table-1)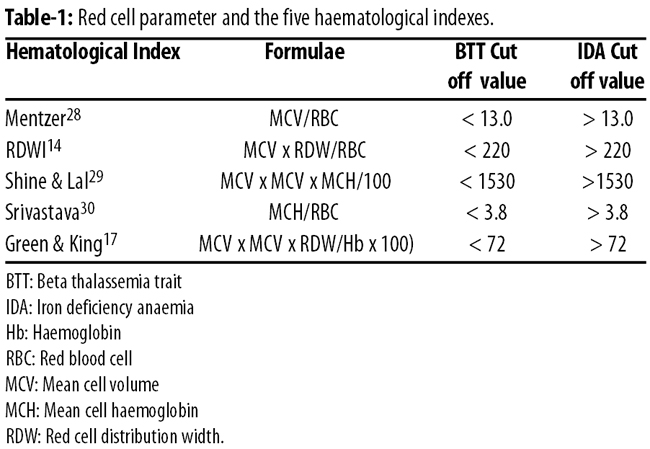
Of the 800 blood samples analyzed, 570(71.3%) were labeled IDA after serum iron analysis and 230(28.8%) isolates as BTT after Hb electrophoresis (Table-2)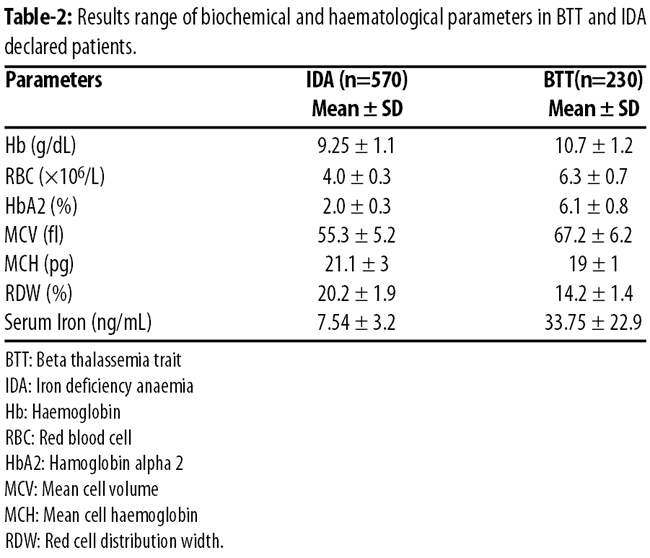
RDW Index (RDWI) established the highest sensitivity and specificity of 100% and 93% respectively. Not a single index provided 100% sensitivity and specificity (Figure-1)
The highest diagnostic values based on the area under the ROC curve were related to the RDWI (Figure-2)
Discussion
Pakistan, an agricultural country, is struggling to defeat IDA, the most prevalent nutritional deficiency all over the globe. In Pakistan, prevalence of IDA among child-bearing age women is 50%, in children it is 65-78% while about 39% of adolescents are suffering from this deficiency.11
The two most common aetiologies of microcytic anaemia i.e., BTT and IDA, are seen in both children and adults. It is mandatory to differentiate BTT from IDA, because diagnosis of BTT often becomes confusing due to its overlapping and similar features with IDA in routine laboratory results.24 However, the prognosis, causes and treatment of these clinical conditions are entirely different.22 There are several similarities in red cell indices of these two groups, for instance reduced Hb, MCV, MCH, microcytosis and hypochromia.14,25
A number of RBC indices and formule have been devised.The purpose of this study was to pick the most accurate formula which could show highest sensitivity and specificity in discriminating BTT from IDA.This formula would help to classify the patients with hypochromic microcytic anaemia into two most important categories, so specific tests can be asked for i.e., serum iron (SI) or Hb electrophoresis. It will save time and reduce diagnostic expenses.26,27
Different mathematical formulae based on red cell indices have been used by researchers to differentiate BTT from IDA, but none has been found to be 100% sensitive and specific. In this study, we checked the sensitivity, specificity, PPV and NPV of various RBC indices-based formulae. We applied five formulae on each enrolled case of microcytic hypochromic sample to differentiate BTT from IDA.14,17,28-30
RDWI index came up with the most dependable index with sensitivity of 100% and specificity of 93%. Our results are consistent with previous studies which showed that RDWI is the most reliable formula to differentiate these two conditions.23,24,31
A Spanish group of haematologists also reported RDWI as the most reliable index.15 A study32 reported Shine and Lal formula as the best index for BTT, although in our study Shine & Lal had 100% sensitivity but only 39% specificity.
One study.33 suggested that Green & King\\\'s index is the best discriminator, but in our study it was the second best index after RDWI. Another study found that formulae presented by Shine and Lal, Srivastava and Mentzler had good discriminative function.34
Many studies have shown that these formulae are only 61-91% successful in properly classifying whether hypochromic and microcytic anaemia is due to BTT or IDA. All the formulae showed overlapping results.26 These results could be due to different values in different studies so there is a need to define separate cut-off values for each population.
We recommend future studies with a larger sample size to accurately determine the sensitivity and sensitivity of various formulae in discriminating BTT from IDA.
Conclusion
RDWI appeared to be the most reliable formula in differentiating BTT from IDA in patients with hypochromic microcytic anaemia. For mass screening of microcytic hypochromic anaemia, this formula can be used in areas lacking facilities for Hb electrophoresis.
Acknowledgment
We are grateful to the Pathology Department of Gomal Medical College and Hayat Medical Laboratory, Dera Ismail Khan, for their support and technical assistance.
Disclaimer: None.
Source of Funding: None.
Conflict of Interest: None.
Reference
1.Wharton BA. Iron deficiency in children: detection and prevention. Br J Haematol 1999; 106: 270-80.
2.Lukens J. The thalassemias and related disorder: an overview. In: Lee R, Foerster J, Lukens J, Paraskevas F, Greer J, Rodgers G, eds. Wintrobe\\\'s clinical hematology. 10th ed Baltimore: Lippincott Williams & Wilkins; 1999.
3.World Health Organization. Assessing the Iron Status of Populations: Report of a Joint World Health Organization/Centers for Disease Control and Prevention Technical Consultation on the Assessment of Iron Status at the Population Level, Geneva, Switzerland, 6-8 April 2004: World Health Organization, Department of Nutrition for Health and Development; 2005.
4.Scholl TO. Iron status during pregnancy: setting the stage for mother and infant.Am J Clin Nutr. 2005;81:1218S-22S.
5.Halterman JS, Kaczorowski JM, Aligne CA, Auinger P, Szilagyi PG. Iron deficiency and cognitive achievement among school-aged children and adolescents in the United States. Pediatrics. 2001;107:1381-6.
6.Bothwell TH, CharltonRW. Iron deficiency in women.A report of the International Nutritional anaemia Consultative Group (INACG). Washington DC:1981; pp 1-68.
7.World Health Organization. Management of birth defects and haemoglobin disorders: Report of a joint WHO-March of Dimes Meeting. Geneva:World Health Organization; 2006.
8.Rund D, Rachmilewitz E. b-Thalassemia. New Engl J Med 2005; 353: 1135-46. Doi: http://dx.doi.org/ 10.1007/springerreference_39844
9.Weatherall D, Clegg J. Inherited haemoglobin disorders: an increasing global health problem. Bull World Health Organ. 2001;79:704-12.
10.Angastiniotis M, Modell B. Global epidemiology of hemoglobin disorders. Ann N Y Acad Sci. 1998;850:251-69. Doi: http://dx.doi.org/10.1111/j.1749-6632.1998.tb10482.x
11.Ansari SH, Shamsi TS, Ashraf M, Farzana T, Bohray M, Perveen K, et al. Molecular epidemiology of b-thalassemia in Pakistan: Far reaching implications. Ind J Hum Genet. 2012;18:193.doi: http://dx.doi.org/10.4103/0971-6866.100762
12.Khattak MF, Saleem M. Prevalence of heterozygous b-thalassaemia in the northern areas of Pakistan. J Pak Med Assoc. 1992;42:32-4.
13.Thomas C, Thomas L. Biochemical markers and hematologic indices in the diagnosis of functional iron deficiency. Clin chemistry. 2002;48:1066-76. doi: http://dx.doi.org/10.2298/jmh0403235t
14.Jayabose S, Giamelli J, Levondoglu Tugal O, Sandoval C, Ozkaynak F, Visintainer P. Differentiating iron deficiency anemia from thalassemia minor by using an RDW-based index. J Pediatr Hematol Oncoly. 1999;21:314.
15.Urrechaga E, Borque L, Escanero JF. The role of automated measurement of RBC subpopulations in differential diagnosis of microcytic anemia and b-thalassemia screening. Amn J Clin Pathol. 2011;135:374-9. doi: http://dx.doi.org/10.1309/ajcpjrh1i0xtnfga
16.Mosca A, Paleari R, Ivaldi G, Galanello R, Giordano P. The role of haemoglobin A2 testing in the diagnosis of thalassaemias and related haemoglobinopathies. J Clin Pathol. 2009;62:13-7. doi: http://dx.doi.org/10.1136/jcp.2008.056945
17.Green R, King R. A new red cell discriminant incorporating volume dispersion for differentiating iron deficiency anemia from thalassemia minor. Blood cells. 1988;15:481-91; discussion 92-5.
18.Ricerca B, Storti S, d\\\'Onofrio G, Mancini S, Vittori M, Campisi S, et al. Differentiation of iron deficiency from thalassaemia trait: a new approach. Haematologica. 1986;72:409-13.doi: http://dx.doi.org/ 10.1016/s0140-6736(73)91446-3
19.Sirdah M, Tarazi I, Al Najjar E, Al Haddad R. Evaluation of the diagnostic reliability of different RBC indices and formulas in the differentiation of the b-thalassaemia minor from iron deficiency in Palestinian population. Int J Lab Hematol. 2008;30:324-30.doi:http://dx.doi.org/10.1111/j.1751-553x.2007.00966.x
20.Ehsani M, Shahgholi E, Rahiminejad M, Seighali F, Rashidi A. A new index for discrimination between iron deficiency anemia and beta-thalassemia minor: results in 284 patients. Pak J Biological Sci. 2009;12:473-5. doi: http://dx.doi.org/10.3923/pjbs.2009.473.475
21.Telmissani OA, Khalil S, Roberts GT. Mean density of hemoglobin per liter of blood: a new hematologic parameter with an inherent discriminant function. Lab Hematology. 1999;5:149-52.
22.Vehapoglu A, Ozgurhan G, Demir AD, Uzuner S, Nursoy MA, Turkmen S, et al. Hematological indices for differential diagnosis of beta thalassemia trait and iron deficiency anemia. Anemia. 2014; 2014. doi: http://dx.doi.org/10.1155/2014/576738
23.Demir A, Yarali N, Fisgin T, Duru F, Kara A. Most reliable indices in differentiation between thalassemia trait and iron deficiency anemia. Pediatr Int. 2002; 44: 612-6. doi: http://dx.doi.org/ 10.1203/00006450-201011001-00837
24.Adlekha S, Chadha T, Jaiswal RM, Singla A. Screening of ?-thalassaemia trait by means of red cell indices and derived formulae. Med J Dr DY Patil University. 2013;6:71. doi: http://dx.doi.org/10.4103/0975-2870.108649
25.Matos JF, Borges KB, Fernandes APS, Faria JR, Carvalho MdG. RDW as differential parameter between microcytic anemias in" pure" and concomitant forms. J Brasileiro de Patologia e Medicina Laboratorial. 2015; 51: 22-7. doi: http://dx.doi.org/10.5935/1676-2444.20150005
26.Miri-Moghaddam E, Sargolzaie N. Cut off determination of discrimination indices in differential diagnosis between iron deficiency anemia and b-thalassemia minor. Int J Hematol-oncolStem Cell Research. 2014;8:27.
27.Ntaios G, Chatzinikolaou A, Saouli Z, Girtovitis F, Tsapanidou M, Kaiafa G, et al. Discrimination indices as screening tests for b-thalassemic trait. Ann hematol. 2007;86:487-91. doi: http://dx.doi.org/10.1007/s00277-007-0371-x
28.Mentzer W. Differentiation of iron deficiency from thalassaemia trait. Lancet. 1973; 301(7808): 882. doi: http://dx.doi.org/10.1016/ s0140-6736(73)91446-3.
29.Shine I, Lal S. A strategy to detect beta-thalassaemia minor. Lancet. 1977;1(8013):692-4. doi: http://dx.doi.org/10.1016/s0140-6736(77)92128-6.
30.Srivastava P, Bevington J. Iron deficiency and/or Thalassaemia trait. Lancet. 1973; 301(7807):832.
31.Niazi M, Tahir M, e Raziq F, Hameed A. Usefulness of Redcell Indices in Differentiating Microcytic Hypochromic Anemias. Gomal J Med Sci. 2010;8(2).
32.Lafferty JD, Crowther MA, Ali MA, Levine M. The evaluation of various mathematical RBC indices and their efficacy in discriminating between thalassemic and non-thalassemic microcytosis. Am J Clin Pathol. 1996;106:201-5. doi: http://dx.doi.org/10.1093/ajcp/106.2.201
33.Okan V, Cigiloglu A, Cifci S, Yilmaz M, Pehlivan M. Red cell indices and functions differentiating patients with the ?-thalassaemia trait from those with iron deficiency anaemia. J Int Med Research. 2009;37:25-30. doi: http://dx.doi.org/10.1177/147323000903700103
34.Rathod DA, Kaur A, Patel V, Patel K, Kabrawala R, Patel V, et al. Usefulness of cell counter-based parameters and formulas in detection of ?-thalassemia trait in areas of high prevalence. Am J Clin Pathol. 2007;128:585-9. doi: http://dx.doi.org/10.1016/s1077-9108(08)79066-2.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: