
Khalida Iqbal ( Department of Biological and Biomedical Sciences, Karachi, Pakistan. )
Najmul Islam ( Department of Medicine, Aga Khan University, Karachi, Pakistan. )
Naseema Mehboobali ( Department of Biological and Biomedical Sciences, Karachi, Pakistan. )
Ali Asghar ( Department of Medicine, Aga Khan University, Karachi, Pakistan. )
Mohammad Perwaiz Iqbal ( Department of Biological and Biomedical Sciences, Karachi, Pakistan. )
December 2016, Volume 66, Issue 12
Original Article
Abstract
Objective: An association between serum levels of vitamin D and glycaemic control in type-2 diabetes mellitus (DM) patients has been reported in some of the studies carried out in the West. However, there are no reports on this relationship in Pakistani diabetic patients. The aim of this study was to ascertain whether vitamin D levels have any influence on glycaemic control in Pakistani patients with type-2 DM.
Methods: In a cross-sectional survey, relationship between serum levels of 25-hydroxy vitamin D (25(OH)D) and glycated haemoglobin (HbA1C) was examined in 141 type-2 diabetic patients including 102 males and 39 females; age range 22 to 70 years, visiting the Aga Khan University Hospital during July 2013-April 2014. Venous blood was collected and analyzed for serum/plasma levels of 25(OH)D and related biomarkers using kit methods. HbA1C levels <7.0% and >7.0% were taken as indicators of good and poor glycaemic control, respectively. An association between 25(OH)D and HbA1C was investigated using regression analysis.
Results: Percent vitamin D deficiency (serum level of 25(OH)D < 20 ng/ml) was significantly higher in patients with poor glycaemic control compared to patients with good glycaemic control (58.7% vs. 30.6%; p-value=0.006). Binary logistic regression analysis revealed positive association between vitamin D deficiency and poor glycaemic control while adjusting for BMI, serum levels of albumin, alanine aminotransferase and alkaline phosphatase (OR, 4.86 (95% CI, 1.9-11.9; p-value<0.001).
Conclusion: The association between vitamin D deficiency and abnormal HbA1C in Pakistani diabetic patients is suggestive that patients with hypovitaminosis D could benefit from vitamin D supplementation.
Keywords: Vitamin D deficiency, Glycaemic control, Diabetes mellitus, HbA1C. (JPMA 66: 1562; 2016)
Introduction
In recent years, a few studies, mostly carried out in the West, have shown an association between hypovitaminosis D [serum levels of 25-hydroxy vitamin D less than 20ng/ml] and abnormal glycated haemoglobin (HbA1C) levels in patients with type II diabetes mellitus.1-6 This association was observed even in the South Asian patients of type-2 diabetes mellitus (DM) living in the United Kingdom (UK).7 However, there are hardly any studies carried out in South Asia to ascertain this relationship. Since HbA1C is a marker of glycaemic control in patients with DM,8 we embarked on investigating the relationship between serum levels 25-hydroxy vitamin D [25(OH)D] and concentration of HbA1C in Pakistani patients with type-2 DM.
Methods
In a cross-sectional survey, 165 consecutive diabetic patients with age ranging from 22 to 70 years visiting the Endocrinology Clinic of the Aga Khan University Hospital between July, 2013 to April, 2014 were enrolled with informed consent. These patients had been diagnosed to have type-2 DM as per guidelines of International Diabetes Federation, which included clinical history and fasting serum glucose concentration >126mg/dl.9 They had not received any vitamin D supplementation during the past 6 months and were free from any of the chronic diseases such as liver disease, uraemia, cancer or lung disease. The study had the approval from the Ethics Review Committee of the Aga Khan University. Medical records of these patients were obtained and those whose HbA1C levels were done within one week of their recruitment were included in this study. One hundred and forty one patients including 102 males and 39 females fulfilled the criterion and were selected for analysis of 25(OH)D and other related biomarkers.
Ten ml blood with at least 4 hours of fasting was collected and serum was analyzed for 25(OH)D, parathyroid hormone (PTH), calcium, alkaline phosphatase (ALP), phosphate, albumin, alanine aminotransferease (ALT) and creatinine using kit methods (Roche Diagnostics, Indianapolis, IN). For statistical analysis of the data, patients were divided into 2 groups on the basis of their glycaemic control: Good glycaemic control (HbA1C <7.0%) and poor glycaemic control (HbA1C >7.0%) as per guidelines of American Diabetes Association.10 Demographic and clinical characteristics in these groups were compared using statistical tests such as chi-square for comparing proportions and Independent sample t test for comparing mean values. Binary logistic regression was applied to study the association between hypovitaminosis D and its relationship with poor glycaemic control. Pearson\\\'s correlation was used for correlation between serum levels of 25(OH)D and concentrations of HbA1C. A p-value of <0.05 was considered significant.
Results
A comparison of demographic characteristics and mean concentrations of biomarkers in patients with good glycaemic control and patients with poor glycaemic control indicates no statistically significant difference with respect to gender, sunlight exposure, age, age of diagnosis, body mass index (BMI), waist circumference, serum levels of calcium, PTH, phosphate, albumin, ALT and creatinine (Table-1)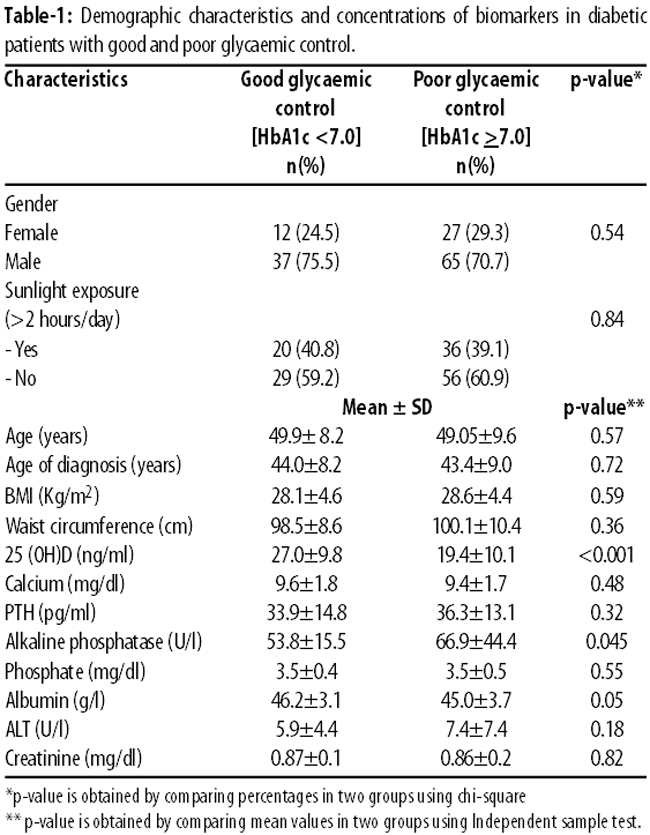
However, mean serum level of 25(OH)D was significantly higher in the group with good glycaemic control compared to the mean level in the group with poor glycaemic control (27.0±9.8 vs. 19.4±10.1ng/ml; p-value <0.001; Table-1). On the other hand, mean serum concentration of ALP was significantly lower in the group of patients with good glycaemic control compared to the group with poor glycaemic control (54±16 vs. 67±44 U/l; p-value = 0.045). Percent vitamin D deficiency (serum 25(OH)D <20ng/ml) was significantly higher in patients with poor glycaemic control than patients with good glycaemic control (58.7% vs. 30.6%, p-value = 0.002; Table-2)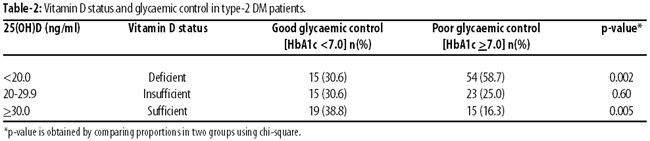
Pearson\\\'s correlation analysis indicated that serum 25(OH)D levels were inversely correlated with concentrations of HbA1C in these patients (r = -0.203; p-value = 0.016). Binary logistic regression analysis revealed association of hypovitaminosis D with poor glycaemic control (odds ratio (OR), 3.22 (95% CI, 1.54-6.7); p-value=0.002; Table-3)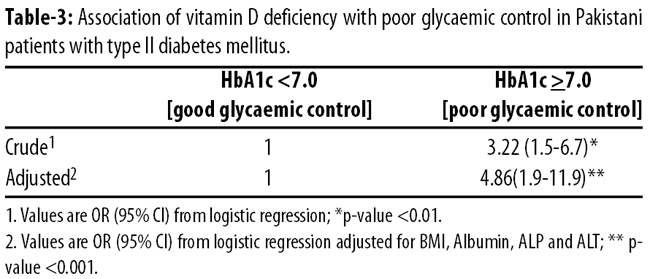
Odds of poor glycaemic control in these diabetic patients was nearly 5-fold when the model was adjusted for other covariates, BMI, serum concentrations of albumin, ALT and ALP (OR, 4.86 (95% CI, 1.9-11.9); p-value <0.001; Table-3).
Discussion
Pakistani population has high prevalence of type-2 DM and vitamin D deficiency.11,12 Because of poor glycaemic control, many of the diabetics develop microvascular complications (retinopathy, nephropathy and neuropathy) and macrovascular problems (cardiovascular disease) leading to increased morbidity and mortality.13-15 Therefore, glycaemic management of type-2 DM patients is of utmost importance to prevent long-term complications. Since HbA1C has emerged as a major biomarker for monitoring glycaemia, it is widely used in the management of diabetic patients.16,17 The newly found relationship of vitamin D and calcium homeostasis with glycaemia and type-2 DM has been of immense help in the control of glycaemia in such patients.18,19 The inverse association of serum levels of 25(OH)D and HbA1C has been reported in a number of observational studies carried out in European countries such as, Italy,1 France,2 Norway,3 Spain,5 Greece,6 UK,7 and the United States of America.4
There are only a few studies carried out on this subject in Asian countries such as, Lebanon19 and Egypt.20 All these studies report an inverse association between vitamin D deficiency and HbA1C levels in population of their type-2 DM patients, and lead to the notion that vitamin D supplementation in these patients should improve their glycaemic control. However, some of trials failed to show any significant improvement in glycaemic control following vitamin D supplementation. For example, in a systematic review of 15 trials, vitamin D supplementation appeared to have no significant effect on HbA1C levels in diabetic patients.21 Nonetheless, conclusions of this review could be questioned on the fact that it included only 4 studies in which HbA1C was measured as a glycaemic control. Another trial carried out in Denmark showed that improved vitamin D status was not associated with HbA1C but insulin secretion did appear to increase in patients with type-2 DM.22 In a study carried out on South Asian type-2 DM patients (n=52) residing in UK, combined oral vitamin D3 and calcium supplementation resulted in a significant decrease in HbA1C.23
Conversely, in three British Asians with type-2 DM, supplementation with vitamin D led to deterioration of glycaemic control.24 In a recent report, Sheth et al have shown lack of association between serum levels of 25(OH)D and HbA1C in 429 type-2 DM patients from Western India.25 However, the mean age of their type-2 DM patients was about 57 years as compared to 49 years in our study and the possibility that this association between 25(OH)D and glycaemic control could be affected by old age in certain populations cannot be discounted. Such a notion is further supported by Mehta et al who have reported lack of association between severity of vitamin D deficiency and elevated levels of HbA1C in elderly diabetic patients in nursing homes.26
To the best of our knowledge, our observation that there is a direct relationship of hypovitaminosis D with poor glycaemic control is the first comprehensive report on this subject in Pakistani diabetic patients. Although Magsi et al have also reported negative association of vitamin D deficiency with plasma levels of glucose, yet their study involved only 13 patients with diabetes mellitus.27 Moreover, they did not use HbA1C as a marker of glycaemia.
The mechanism by which vitamin D could be influencing glucose metabolism in diabetic patients include: improvement in insulin sensitivity and b cell survival;18 increased insulin secretion from pancreatic b cells28 and regulation of calcium flux for normalization of glucose tolerance and protection of beta cells against cytokine-induced apoptosis.18
The present study also had certain limitations. Being a cross-sectional survey, it could not indicate the cause and effect relationship. Moreover, we did not monitor HOMA-IR (Homeostasis model assessment for insulin resistance) for its association with 25(OH)D in our type-2 DM patients.
In spite of these limitations, the data did provide evidence regarding the role of vitamin D in glycaemic control in Pakistani diabetic patients. Large intervention trials using vitamin D supplementation in type-2 DM patients will be required to provide further evidence that Pakistani patients can benefit from vitamin D supplements in improving glycaemic control, thereby attenuating diabetic complications.
Conclusion
The association of vitamin D deficiency with poor glycaemic control in Pakistani patients with type-2 DM points towards the role vitamin D supplementation could possibly play in regulation of glycaemia in these patients.
Acknowledgement
We gratefully acknowledge the help provided by Ms. Shaheena Anwar in regression analysis. The study was supported by a grant [PSF/Res/S-AKU/Med (336)] by the Pakistan Science Foundation.
References
1.Zoppini G, Galletti A, Targher G, Brangani C, Pichiri I, Negri C, et al. Glycated haemoglobin is inversely related to serum vitamin D levels in type 2 diabetic patients. PLoS One. 2013; 8:e82733.
2.Kajbaf F, Mentaverri R, Diouf M, Fournier A, Kamel S, Lalau JD. The Association between 25-Hydroxyvitamin D and Hemoglobin A1c Levels in Patients with Type 2 Diabetes and Stage 1-5 Chronic Kidney Disease. Int J Endocrinol. 2014; 2014:142468.
3.Hutchinson MS, Figenschau Y, Njølstad I, Schirmer H, Jorde R. Serum 25-hydroxyvitamin D levels are inversely associated with glycated haemoglobin (HbA(1c)). The Tromsø Study. Scand J Clin Lab Invest. 2011; 71:399-406.
4.Kositsawat J, Kuchel GA, Tooze JA, Houston DK, Cauley JA, Kritchevsky SB, et al. Vitamin D insufficiency and abnormal hemoglobin a1c in black and white older persons. J Gerontol A Biol Sci Med Sci. 2015; 70:525-31.
5.Miñambres I, Sánchez-Quesada JL, Vinagre I, Sánchez-Hernández J, Urgell E, de Leiva A, et al. Hypovitaminosis D in type 2 diabetes: relation with features of the metabolic syndrome and glycemic control. Endocr Res. 2015; 40: 160-5.
6.Kostoglou-Athanassiou I, Athanassiou P, Gkountouvas A, Kaldrymides P. Vitamin D and glycemic control in diabetes mellitus type 2. Ther Adv Endocrinol Metab. 2013; 4: 122-8.
7.Tahrani AA, Ball A, Shepherd L, Rahim A, Jones AF, Bates A. The prevalence of vitamin D abnormalities in South Asians with type 2 diabetes mellitus in the UK. Int J Clin Pract. 2010; 64: 351-5.
8.Syed IA. Glycated haemoglobin; past, present, and future are we ready for the change. J Pak Med Assoc. 2011; 61: 383-8.
9.International Diabetes Federation. Screening and diagnosis. In: Global Guidelines for Type 2 Diabetes. International Diabetes Federation; 2012, pp 9-14.
10.American Diabetes Association. Glycemic Targets. Sec. 6. Standards of Medical Care in Diabetes. Diabetes Care. 2015; 38:S33-S40.
11.Shera AS, Jawad F, Maqsood A. Prevalence of diabetes in Pakistan. Diabetes Res Clin Pract. 2007; 76:219-22.
12.Mehboobali N, Iqbal SP, Iqbal MP. High prevalence of vitamin D deficiency and insufficiency in a low income peri-urban community in Karachi. J Pak Med Assoc. 2015; 65: 946-59.
13.Raman R, Gupta A, Krishna S, Kulothungan V, Sharma T. Prevalence and risk factors for diabetic microvascular complications in newly diagnosed type II diabetes mellitus. Sankara Nethralaya Diabetic Retinopathy Epidemiology and Molecular Genetic Study (SN-DREAMS, report 27). J Diabetes Complications. 2012; 26: 123-8.
14.Girach A, Manner D, Porta M. Diabetic microvascular complications: can patients at risk be identified? A review. Int J Clin Pract. 2006; 60: 1471-83.
15.Mata-Cases M, De Prado-Lacueva C, Salido-Valencia V, Fernández-Bertolín E, Casermeiro-Cortés J, García-Durán M, et al. Incidence of complications and mortality in a type 2 diabetes patient cohort study followed up from diagnosis in a primary health care centre. Int J Clin Pract. 2011; 65: 299-307.
16.Manley S. Haemoglobin A1c--a marker for complications of type 2 diabetes: the experience from the UK Prospective Diabetes Study (UKPDS). Clin Chem Lab Med. 2003; 41: 1182-90.
17.Sato A. [Indicators of glycemic control --hemoglobin A1c (HbA1c), glycated albumin (GA), and 1,5-anhydroglucitol (1,5-AG)]. Rinsho Byori. 2014; 62: 45-52.
18.Pittas AG, Lau J, Hu FB, Dawson-Hughes B. The role of vitamin D and calcium in type 2 diabetes. A systematic review and meta-analysis. J Clin Endocrinol Metab. 2007; 92: 2017-29.
19.Ahmadieh H, Azar ST, Lakkis N, Arabi A. Hypovitaminosis D in patients with type 2 diabetes mellitus: a relation to disease control and complications. ISRN Endocrinol. 2013; 2013: 641098.
20.Abeer A. AL-Refai, Tawfeeq AR. Study of Serum 25-hydroxyvitamin D Status and Glycemic Control in Diabetic Patients. J Am Science 2013; 9:277-86.
21.George PS, Pearson ER, Witham MD. Effect of vitamin D supplementation on glycaemic control and insulin resistance: a systematic review and meta-analysis. Diabet Med. 2012; 29: e142-50.
22.Kampmann U, Mosekilde L, Juhl C, Moller N, Christensen B, Rejnmark L, et al. Effects of 12 weeks high dose vitamin D3 treatment on insulin sensitivity, beta cell function, and metabolic markers in patients with type 2 diabetes and vitamin D insufficiency - a double-blind, randomized, placebo-controlled trial. Metabolism. 2014; 63:1115-24.
23.Sabherwal S, Bravis V, Devendra D. Effect of oral vitamin D and calcium replacement on glycaemic control in South Asian patients with type 2 diabetes. Int J Clin Pract. 2010; 64:1084-9.
24.Taylor AV, Wise PH. Vitamin D replacement in Asians with diabetes may increase insulin resistance. Postgrad Med J. 1998; 74:365-6.
25.Sheth JJ, Shah A, Sheth FJ, Trivedi S, Lele M, Shah N, et al. Does vitamin D play a significant role in type 2 diabetes? BMC Endocr Disord. 2015; 15: 5.
26.Mehta M, Tommasulo B, Pekmezaris R, Kozikowski A, Akerman M, Karim N, et al. SAT-0234:Association Between Vitamin D Deficiency and HbA1C Levels in Elderly Patients with Type 2 Diabetes in Long Term Care Institutions. Vitamin D Metabolism & Action. Endocrine Society\\\'s 96th Annual Meeting and Expo, June 21-24, 2014 - Chicago.
27.Magsi MA, Ijaz A, Maryam A, Yousaf S, Sana F, Najamuddin. Vitamin D status and diabetes mellitus. Professional Med J. 2014; 21:445-9.
28.Zeitz U, Weber K, Soegiarto DW, Wolf E, Balling R, Erben RG. Impaired insulin secretory capacity in mice lacking a functional vitamin D receptor. FASEB J. 2003; 17:509-11.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: