
Zafar Ullah ( Department of Rheumatology, Shifa International Hospital, Islamabad, Pakistan. )
Zain Ul Abideen ( Department of Internal Medicine, Shifa International Hospital, Islamabad, Pakistan. )
Raja Farhat Shoaib ( Department of Neurology, Shifa International Hospital, Islamabad, Pakistan. )
Arsalan Ahmad ( Department of Neurology, Shifa International Hospital, Islamabad, Pakistan. )
Qamar Zaman ( Department of Neurology, Shifa International Hospital, Islamabad, Pakistan. )
Rashid Nazir ( Department of Radiology, Shifa International Hospital, Islamabad, Pakistan. )
November 2016, Volume 66, Issue 11
Case Reports
Abstract
Eosinophilic granulomatosis with polyangiitis also known as Churgg-Strauss syndrome is a systemic multi system vasculitis. Neurological involvement is mostly in the form of peripheral nervous system disease. Central nervous system involvement is relatively uncommon with most cases being secondary to ischaemic infarctions. Intra cerebral haemorrhage is rare and is usually in the form of solitary haemorrhagic lesions. Multiple intra cerebral haemorrhages are exceptionally rare with only one case documented in medical literature. Here, we present the case of a middle aged male who presented to us with multiple intra cerebral haemorrhages, mono neuritis multiplex, renal and respiratory tract involvement and peripheral blood eosinophilia. Upon fulfilling the American College of Rheumatology criteria, he was diagnosed as an exceptionally rare case of EGPA with multiple intra cerebral haemorrhages. He was treated with intra venous corticosteroids and immune suppressants, and made a good recovery.
Keywords: Eosinophilic granulomatosis with polyangiitis, Churgg-Strauss syndrome, Multiple intracerebral haemorrhages.
Introduction
Eosinophilic granulomatosis with polyangiitis (EGPA) is an autoimmune disorder characterized by necrotizing eosinophilic vasculitis of medium and small sized blood vessels.1 It is a multi-system disorder involving the respiratory, cardiovascular, gastro intestinal, nervous systems and the skin.2 The diagnosis is based on the American College of Rheumatology (ACR) criteria which has a sensitivity of 85% and a specificity of 99.7% when 4 or more of the following six criteria are met ; presence of asthma , blood eosinophilia , mono or polyneuropathies , non-fixed pulmonary infiltrates, paranasal sinus abnormalities and demonstration of extravascular eosinophils in a biopsy specimen.2
The peripheral nervous system is more commonly involved as compared to the central nervous system.This may be in the form of sub arachnoid haemorrhage, cerebral infarction and haemorrhagic strokes.3 The later complication has been reported very rarely.
The case of a middle aged male with a long standing history of asthma and para nasal sinusitis presenting with sudden onset limb weakness is reported. He had multiple intra cerebral haemorrhages and was later diagnosed with EGPA.
Case Report
A 57 year old gentleman with a history of late onset bronchial asthma for five years, para nasal sinusitis, hypertension and hypercholesterolaemia presented to our hospital\\\'s emergency in May 2015 with sudden onset weakness in the left arm and leg, accompanied with confusion. This was preceded by nausea and vomiting .He had a similar episode 3 months back involving the right side of his body for which he had sought no treatment and it improved with time. He also had urinary and faecal incontinence at presentation.
He had been unwell for the past 3 months and had anorexia, weight loss of 6 kilograms and progressive gait difficulty. His son described that he had started to drag his right foot while walking for the past few months. He was a chronic smoker of 20 cigarettes / day.
On examination, he was a middle aged male, confused and did not follow single step commands. His pulse was 90 per minute and regular, blood pressure 130/90 mmHg, respiratory rate 25 / minute and was afebrile.He had a Glasgow Comma scale (GCS) of 14/15.
There were no speech or cranial nerve abnormalities. Muscle power was graded as 1/5 in all muscles of the left upper and lower limb accompanied by brisk deep tendon reflexes (DTR) and an extensor plantar response. Power on the right side was 5/5 with normal DTR and flexor plantar response. There were no cerebellar signs or gross sensory abnormalities.Fundsocopy was normal.
Examination of the cardiovascular system was unremarkable. Respiratory examination revealed widespread wheeze heard in all lung zones bilaterally.
Laboratory tests performed in the emergency are summarized in Table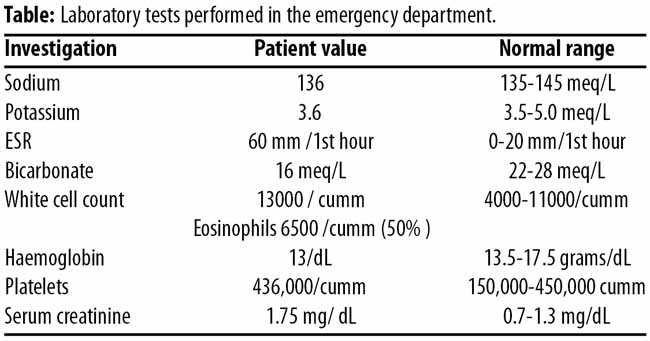
A Computed tomogram (CT) scan was performed in the emergency as shown in Figure-1A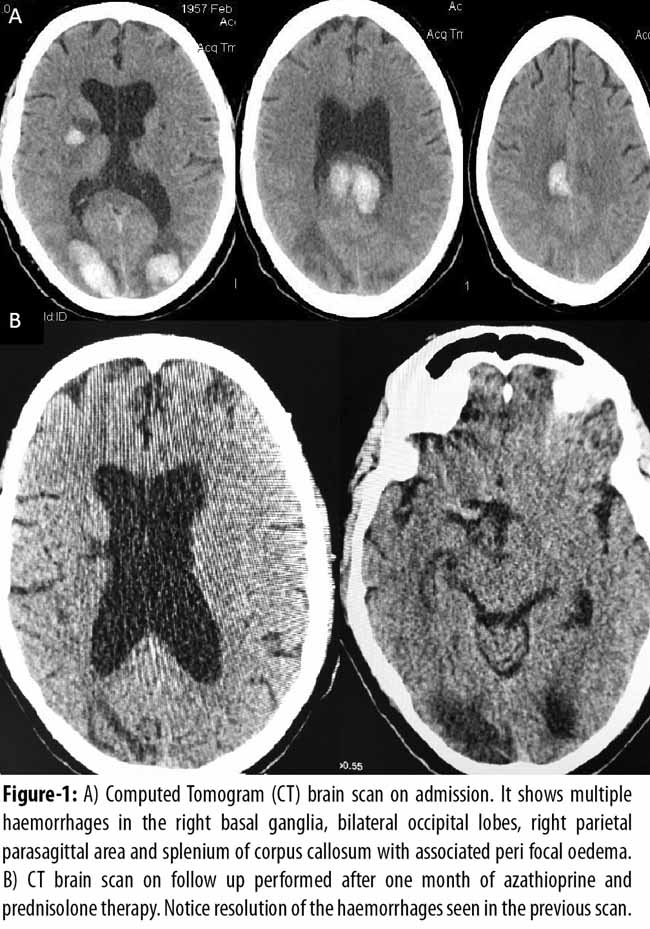
There were multiple haemorrhages in the right basal ganglia, bilateral occipital lobes, right parietal parasagittal area and splenium of corpus callosum with associated peri focal oedema.
Patient was admitted to our stroke unit for suspected vasculitis.The erythrocyte sedimentation rate (ESR) was 60 mm/1st hour and peri nuclear anti neutrophil cytoplasmic antibody (pANCA) antibodies were positive to a level of 90%. The chest X- ray did not reveal any changes.
A nerve conduction study (NCS) and electromyography (EMG) was done for the right sided foot drop and showed severe motor sensory axonal polyneuropathy affecting the legs more than the arms and right more than the left side with ongoing active denervation.
A rheumatology opinion was sought and the patient was diagnosed as a case of EGPA. He was given methyl prednisolone one gram intravenously followed by oral prednisolone at 1 mg/kg in tapering doses and azathioprine which was increased to 100 mg twice daily on discharge. He was offered treatment with cyclophosphamide which was refused.
On follow up one month later his hemiparesis had improved. He could now stand up with support and could move his left arm and leg against gravity and moderate resistance. A follow up CT scan of the brain revealed resolution of the intra cerebral haemorrhages with immunosuppressive therapy as shown is Figure-1B. The serum creatinine also decreased to 1.0 mg/dL and he did not suffer any adverse effects of medication.
Informed consent was sought from patient for using his laboratory values and CT scan images for reporting purpose.
Discussion
EGPA has an incidence of 0.5-6.8 per million and a prevalence of 10.7-14 per million.4 It has a prodromal allergic/atopic phase consisting of asthma and rhino sinusitis, an eosinophilic phase involving eosinophilic infiltration of various tissues and a vasculitic phase causing multi system involvement.5 Our patient presented in the vasculitic phase.
EGPA most commonly involves the respiratory tract as non-fixed pulmonary infiltrates and chronic sinusitis while asthma occurs in about 95% patients.5 Our patient had the latter two conditions. Gastro intestinal, renal, cardiac and musculoskeletal systems may be involved.5,6 Our patient had renal involvement reflected by raised serial serum creatinine levels.
Neurological involvement is seen in 60-80% cases of EGPA with a predilection for the peripheral nervous system.1,3 This is usually mono neuritis multiplex. The central nervous system may be involved in 6.3-27.0% of patients. 1,3 Cerebrovascular events have a frequency of 6.2-6.4%.1,3 This involvement is usually in the form of ischaemic infarctions and cognitive decline.
Intra cerebral haemorrhage is a rare occurrence with EGPA. The first case was reported in 1993 by Chang et al.7 We performed a PubMed search and found only eleven cases reported to date and only one, reported by Liou et al in 1997 described multiple intra cerebral haemorrhages. To the best of our knowledge no case has ever been reported from Pakistan.
EGPA is diagnosed using the ACR criteria. Our patient met four of the six criteria including asthma, sinusitis, blood eosinophilia and polyneuropathy. He had a very high pANCA titer which are positive in 75% and 25% of those with and without renal impairment, respectively. In general 40 % of patients with EGPA have positive pANCA antibodies.5
Treatment involves assessing major organ systems involved. Numerous scores are available to predict mortality. The five factor score considers cardiac muscle and vasculature involvement, renal disease, gastro intestinal disease, CNS involvement and proteinurea of greater than 1 gram per day. A FFS of 0 carries a mortality of 11.9 %, 1 carries a mortality of 25.9%, and 2 carries a mortality of 45.956 Our patient scored 2 and had a high predicted mortality demanding urgent and aggressive treatment.
Cyclophosphamide is typically used in combination with glucocorticoids for patients with severe, multi organ disease. The FFS assesses the severity and guides treatment. A FFS of 2 or more, or 1 with cerebral or pulmonary involvement necessitates adding cyclophosphamide. When used with glucocorticoids this decreases mortality compared to using the latter alone.8,9 Our patient had refused cyclophosphamide. Azathioprine is used after induction of remission with cyclophosphamide as a glucocorticoid sparing agent for patients requiring long term therapy.10
It was interesting to observe our patient\\\'s clinical course. Despite having severe disease and a FFS of 2, he responded dramatically without cyclophosphamide. A follow up CT scan of the brain shown in figure 1B, revealed complete remission of the haemorrhages and further confirmed our diagnosis of an immune vasculitis.
Conclusion
EGPA can rarely present as intra cerebral haemorrhage which is usually a solitary lesion. The occurrence of multiple haemorrhages is exceptionally rare and timely recognition and management prevents mortality and morbidity. Our patient had a remarkable response with methylprednisolone and azathioprine without using cyclophosphamide.
Disclaimer: None.
Conflict of Interest: None.
Funding Disclosure: None.
References
1.Mouthon L, Dunogue B, Guillevin L. Diagnosis and classification of eosinophilic granulomatosis with polyangiitis (formerly named Churg-Strauss syndrome). J Autoimmun 2014 ;48-49 :99-103
2.Khoury P , Grayson PC , Klion AD. Eosinophils in vasculitis: characteristics and roles in pathogenesis. Nat Rev Rheumatol 2014; 10: 474-83.
3.Sehgal M, Swanson JW, DeRemee RA, Colby TV. Neurologic manifestations of Churg-Strauss syndrome. Mayo Clin Proc 1995; 70: 337-41
4.Pagnoux C, Guilpain P, Guillevin L. Churg-Strauss syndrome. Curr Opin Rheumatol 2007; 19: 25-32
5.Taormina G, Andolina G, Banco MA, Costanza-Gaglio EJ, Bonura A, Buscemi S. An uncommon presentation of eosinophilic granulomatosis with polyangiitis: a case report. J Med Case Rep 2014; 8:190
6.Cheng MJ, Huang PH, Liao PW, Chen JT, Chiang TR. Multiple cerebral and cerebellar infarcts as the first clinical manifestation in a patient with Churg-Strauss syndrome: case report and literature review. Acta Neurol Taiwan 2012; 2:169-75.
7.Chang Y, Kargas SA, Goates JJ, Horoupian DS. Intraventricular and subarachnoid haemorrhage resulting from necrotizing vasculitis of the choroid plexus in a patient with Churg-Strauss syndrome. Clin Neuropathol 1993;12:84-7
8.Greco A, Rizzo MI, De Virgilio A, Gallo A, Fusconi M, Ruoppolo G,et al. Churg-Strauss syndrome. Autoimmun Rev 2015; 14: 341-8.
9.Cohen P, Pagnoux C, Mahr A, Mouthon L, Le Guern V, André MH, et al; French Vasculitis Study Group Churg-Strauss syndrome with poor-prognosis factors: A prospective multicenter trial comparing glucocorticoids and six or twelve cyclophosphamide pulses in forty-eight patients. Arthritis Rheum 2007; 57: 686-93.
10.Gioffredi A, Maritati F, Oliva A, Buzio C. Eosinophilic Granulomatosis with Polyangiitis: An Overview. Front Immunol 2014; 5: 549.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: