
Safina Ahmed ( DHA Phase-1, Foundation University Medical College, Islamabad. )
Mumtaz Ahmad ( Department of Pathology, Foundation University Medical College, Islamabad. )
March 2016, Volume 66, Issue 3
Original Article
Abstract
Objective: To compare the diagnostic accuracy of touch imprint cytology and frozen section in the diagnosis of malignant breast lumps keeping histopathological diagnosis as the gold standard.
Methods: The cross-sectional validation study was conducted at Foundation University Medical College, Islamabad, from February 2011 to February 2012, and comprised patients undergoing mastectomy/lumpectomy. The specimens were collected from the operation theatre of Fauji Foundation Hospital, Rawalpindi. After tissue fixation, three representative sections were processed and the slides were stained with haematoxylin and eosin stain. The person analysing touch imprint cytology slides was blinded to the frozen section and histopathological slide results and vice-versa. Data was analysed using SPSS 17.
Results: Out of 76 patients with a mean age of 49±15.14 years, 61(80%) were diagnosed with malignant breast diseases. The sensitivity, specificity, positive predictive value, negative predictive value and true positives of touch imprint cytology were 96.72%, 100%, 100%, 88.24% and 96.72% respectively. The corresponding values of the frozen section were 100% each. The diagnostic accuracy calculated for touch imprints and frozen section was 97.37% and 100% respectively.
Conclusion: The diagnostic accuracy of frozen section was better than touch imprint cytology in rapid intra-operative diagnosis. However, touch imprints can safely be used as an alternative intra-operative procedure to ensure satisfactory results.
Keywords: Frozen section, Breast cancer, Accuracy, Sensitivity, Specificity. (JPMA 66: 292; 2016).
Introduction
Breast cancer is a worldwide oncological health problem and the leading cause of women mortality and morbidity.1 Statistics indicate that breast cancer is accountable for one-third of all female cancers.2
According to Surveillance Epidemiology and End Results (SEER) data, 178,480 women were diagnosed with invasive breast cancer, 62,030 with carcinoma in situ, and over 40,000 women died of the disease in 2007 in the United States.3,4 Pakistan tops the Asian countries in terms of prevalence of breast cancer which is 34.6% of all cancer cases among females.5
Two pathological diagnostic approaches are used for breast lesions. Pre-operative diagnostic techniques include fine needle aspiration cytology (FNAC), core-needle biopsy (CNB), and excisional biopsy.6 Intra-operative diagnostic techniques include frozen-section, touch imprint cytology and intra-operative FNAC.7
Intra-operative diagnostic modalities are important in making immediate decisions for the optimal extent of surgery.8 These techniques are also used to assess the status of surgical margins. To minimise the extensive axillary dissection, sentinel lymph node metastases is judged by these techniques.
Although it is established that frozen section is the most reliable intra-operative diagnostic method with the sensitivity, specificity and accuracy of 100%, but the technique is expensive. It requires technical expertise and expensive equipment and is not available in many hospitals, particularly in rural health centres.1,9
Touch imprint cytology is considered a good alternative method with a sensitivity of 92.99%, a specificity of 93.33% and an accuracy of 92.5%.1 It is useful especially in hospitals with limited technical and financial services. Thus, it is a reliable, rapid, relatively safe and cost-effective technique which requires less financial, human and technical facilities.10
The current study was planned to evaluate the diagnostic accuracy of touch imprint cytology and compared it with the frozen-section technique.
Materials and Methods
The cross-sectional validation study was conducted at Foundation University Medical College, Islamabad, from February 2011 to February 2012, and comprised patients undergoing mastectomy/lumpectomy. After approval from the institutional ethics committee, mastectomy/ lumpectomy specimens were collected from the operation theatre of Fauji Foundation Hospital, Rawalpindi. Every specimen was serially sliced and the lesion was identified. The most representative part of the lesion was used. Touch imprint cytology slides were made and stained with haemacolour.
For frozen section, the selected tissue piece was embedded in optimal cutting temperature (OCT) mounting medium and placed in cryostat. The slides were stained with haematoxylin and eosin (H&E) stain. The results of frozen section were conveyed to the surgeon.
After tissue fixation, three representative sections were taken. These were processed and the slides were stained with H&E. The stained sections of breast tissue were examined simultaneously by the two researchers; one of them being a consultant histopathologist.
Selection bias was controlled by selecting a population that met the inclusion and exclusion criteria. All female patients undergoing breast lumpectomies were included in the study. Already diagnosed cases of breast carcinoma and those patients who were undergoing radiotherapy or chemotherapy were not included in the study. The person who reported touch imprint cytology slides was blinded to the frozen section and histopathological slide results and vice-versa. The results of histopathology slides were taken as the gold standard.
Data was analysed using SPSS 17.
Results
Out of 76 patients with a mean age of 49±15.14 years (range: 26-87 years), 61(80%) were diagnosed with malignant breast disease and 15(20%) had benign breast disease.
Among the 61 patients with malignant breast lesions, 53(86%) were diagnosed with invasive ductal carcinoma, 5(8%) invasive lobular carcinoma, 1(2%) patient each for medullary, metaplastic carcinoma and invasive cribriform carcinoma. The range of tumour size in malignant breast cases was recorded (Figure-1).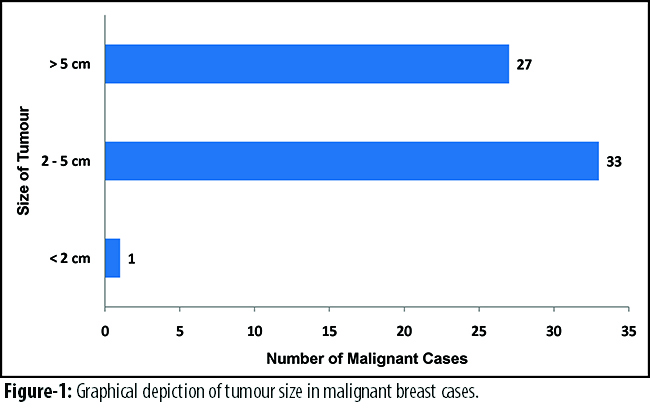
Among 15 cases of benign breast lesions, 7(46%) patients had fibroadenoma, 5(33%) had fibrocystic changes and 1(7%) case each had fat necrosis, duct ectasia and benign phyllodes tumour.
Out of 61 malignant cases, 59(96%) were diagnosed correctly on touch imprint cytology, while 2(4%) were given false negative results. The histology of the false negative cases turned out to be invasive lobular carcinoma (Figure-2)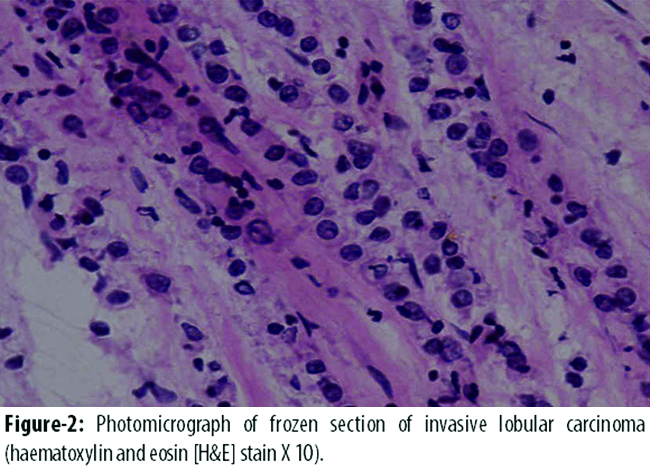
and invasive ductal carcinoma on paraffin section (Figure-3).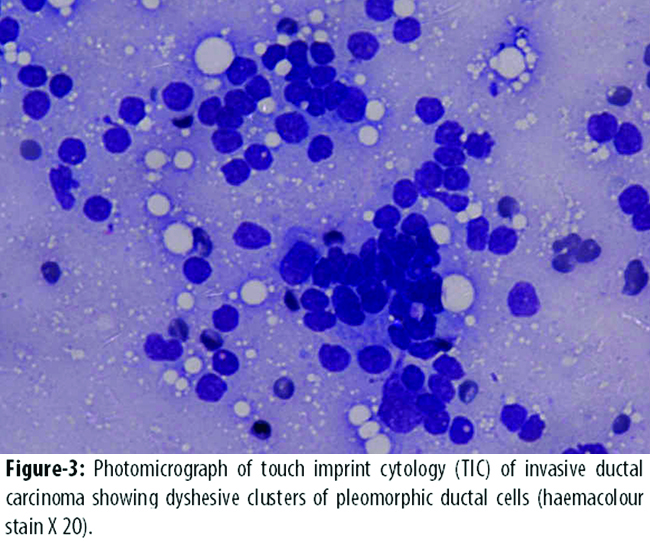
No false positive diagnosis was made on touch imprints. So its specificity and positive predictive value (PPV) turned out to be 100%. However, the sensitivity rate was 96.72% and negative predictive value (NPV) was 88.24%. Hence, the diagnostic accuracy of touch imprint cytology was 97.37%.
All the 61(80%) malignant cases as well as 15(20%) benign cases were diagnosed correctly on frozen section. No false positive or false negative cases were recorded. Therefore, the sensitivity, specificity, PPV, NPV and diagnostic accuracy turned out to be 100%.
Discussion
Frozen-section and touch imprint cytology is performed to confirm the diagnosis of malignancy made on fine-needle aspiration or Tru-Cut biopsy.11 These modalities also help to reach a diagnosis if there was no previous FNAC or CNB result available.12 The frozen section and other intra-operative techniques have also gained popularity in assessing the surgical margins and sentinel lymph node status.13,14
A study done7 on 319 breast cancer patients in Pakistan showed age range between 24 and 90 years (mean age: 53.3 years), which was higher than the current study. The frequency of malignant cases in their study was 89.9% and of benign cases was 9.09%. Another study done in Pakistan15 on breast cancer pattern in 3,431 cases revealed invasive ductal carcinoma to be the most common type of breast cancer.
In the present series, we were able to accurately diagnose 59 malignant cases on touch imprint cytology, while 2 cases were misdiagnosed giving false negative results. These cases were later diagnosed to be invasive lobular carcinoma and invasive ductal carcinoma on paraffin embedded sections. The marked desmoplastic stromal element in these tumours contributed to low cellularity leading to false negative results. The sensitivity, specificity and diagnostic accuracy thus calculated for touch imprint cytology was 96.72%, 100% and 97.37% respectively. The PPV and NPV were 100% and 88.24% respectively.
These results are comparable to a study16 which revealed the sensitivity, specificity and accuracy rates as 100% for class II and class V cytology lesions on touch imprints. Conversely, sensitivity, diagnostic accuracy and NPV were 87%, 95% and 85% respectively for class III and IV lesions.
Another study8 on touch imprints of breast lesions revealed higher sensitivity (100%) and lower specificity (71%) than the present study. These results were obtained when atypia was considered positive for malignancy. The PPV (88%) and diagnostic accuracy (85.55%) rates in this study were lower compared to our study. These values became 100% when atypia was categorised as negative for malignancy rather being positive for malignancy.
In the current study, we were able to accurately diagnose all histologically proven malignant (n=61) as well as benign (n=15) breast cases on frozen section. The sensitivity, specificity and diagnostic accuracy were 100%.
In Egypt, a comparative study1 on 130 patients revealed sensitivity, specificity and accuracy rates of frozen section as 100%. However, their sensitivity and specificity rates of touch imprint cytology were lower than the current study, 92.22% and 93.33% respectively. The NPV and PPV were also lower measuring 80% and 97.65% respectively. The rate of false negative cases was lower while the rate of false positive cases was higher compared to our study.
A study of 319 breast lump cases7 in Karachi revealed sensitivity, specificity, NPV and PPV for frozen section as 99.6%, 93%, 96.6% and 99.3% respectively. The diagnostic yield of frozen section in their series was a bit low compared to our study. The number of discordant cases was 3 in this study; 2 cases were false positive and 1 false negative. The cases in which discrepancy was seen were lymphoma and atypical ductal papilloma.
In another study17 frozen sections accurately diagnosed 623 out of 650 cases. The frozen section diagnosis was deferred to paraffin section in 22 cases. In their study 3 false positive and 24 false negative cases were diagnosed. The sensitivity and specificity recorded in their study was lower compared to our study measuring 91.7% and 99.2% respectively.
One study9 showed almost comparable results to our study. Out of 290 breast cancer patients, frozen section analysis revealed only 2 false negative cases. The diagnosis of phyllodes tumour was missed in these cases. The sensitivity and specificity turned out to be 99.3% and 100% respectively. The PPV was 100%.
Amongst the large series reporting accuracy of frozen section diagnosis in the 1960s and early 1970s, the results were generally excellent giving false positive rates of 0.2-0.3% and false negative rates between 0.5 and 1.2%. On the contrary, the present study has shown 100% results for frozen section giving no false positive or false negative results (Table).
A study conducted18 on 2436 primary breast carcinomas showed an overall decline in the use of frozen sections. Although frozen sections are still popular for assessment of surgical margins as well as for the evaluation of sentinel lymph nodes,19 but cytology and CNB are becoming popular for primary diagnosis.20
Conclusion
The diagnostic accuracy of frozen section was better than touch imprint cytology in making rapid intra-operative diagnosis. However, the touch imprint cytology can be reliably used as an acceptable alternative at centres where frozen section facility is not available.
References
1. El-Bolkainy TM, Shabaan HA, Abodeif WT, El-Bolkainy MN, El-Tony A. Intra-operative diagnosis of breast mass-lesions: Comparison of the validity of touch smear preparation and frozen section techniques. J Egypt Nati Canc Inst 2008; 20: 63-9.
2. Sohail S, Alam SN. Breast Cancer in Pakistan, awareness and early detection, J Coll Physicians Surg Pak 2007; 17: 711-2.
3. Lester SC. The Breast. In: Kumar V, Abbas AK, Fausto N, Aster JC. Robbins and Cotran Pathologic Basis of Disease. 8thed. New Delhi, India: Elsevier, 2010; pp 1065-95.
4. DeSantis C, Siegel R, Bandi P, Jemal A. Breast cancer statistics. CA Cancer J Clin 2011; 61: 409-18.
5. Ahmed F, Mahmood S, Hatcher J, Khan SM. Breast cancer risk factor knowledge among nurses in teaching hospitals of Karachi, Pakistan: A cross-sectional study. BMC Nurs 2006; 5: 6.
6. Rahman MZ, SikderAM, Nabi SR. Diagnosis of breast lump by fine needle aspiration cytology and mammography. Mymensingh Med J 2011; 20: 658-64.
7. Sultana N, Kayani NJ. Validity of frozen section in the diagnosis of breast lumps: 5 years experience at the Aga Khan University Hospital. J Pak Med Assoc 2005; 55: 533-6.
8. Akhtar ZM, Qureshi SA, Aziz N, Niazi S, Qureshi SS, Bukhari MH. Evaluation of accuracy of intra-operative imprint cytology of detection of breast lesions. Ann King Edward Med Coll 2010; 16: 48-54.
9. Bellolio JE, Guzmán GP, Orellana CJ, Roa S JC, Villaseca HM, Araya O JC, et al. Diagnostic value of frozen section biopsy during surgery for breast lesions or neoplasms. Rev Med Chil 2009; 137: 1173-8.
10. Hiregoudar AD, Godhi AS, Malur PR, Gogeri BV, Metgud SC. Accuracy of intra-operative imprint smears in breast tumours: A study of 40 cases with reviw of literature. Indian J Surg 2006; 17: 736-9.
11. Gal AA, Cagle PT. The 100-yearanniversary of the description of the frozen section procedure. JAMA 2005; 294: 3135-7.
12. Frankel PP, Esteves VF, Thuler LC, Vieira RJ. Diagnostic accuracy of the fine needle aspiration cytology and core needle biopsy as a diagnostic method for breast lesions. Rev Bras Ginecol Obstet 2011; 33: 139-43.
13. Valdes EK, Boolbol SK, Ali I, Feldman SM, Cohen JM. Intra-operative touch preparation cytology for margin assessment in breast conservation surgery: Does it work for lobular carcinoma? Ann Surg Oncol 2007; 14: 2940-45.
14. Layfield DM, Agrawal A, Roche H, Cutress RI. Intraoperative assessment of sentinel lymph nodes in breast cancer. Br J Surg 2011; 98: 4-17.
15. Afsar NA, Kulsoom B, Mateen A, Ahmed S, Tahseen M, Ahmed A. Breast cancer pattern and chemotherapy response--an institutional study in Pakistan. Asian Pac J Cancer Prev 2010; 11: 825-30.
16. Bukhari MH, Akhtar ZM. Comparison of accuracy of diagnostic modalities for evaluation of breast cancer with review of literature. Diagn Cytopathol 2009; 37: 416-24.
17. Bianchi S, Palli D, Ciatto S, Galli M, Giorgi D, Vezzosi V, et al . Accuracy and reliability of frozen section diagnosis in a series of 672 nonpalpable breast lesions. Am J Clin Pathol 1995; 103: 199-205.
18. Manfrin E, Remo A, Falsirollo F, Pollini GP, Parisi A, Nottegar A, et al. Intra operative frozen section technique for breast cancer: end of an era. Pathologica 2011; 103: 325-30.
19. Taffurelli M, Montroni I, Santini D, Fiacchi M, Zanotti S, Ugolini G, et al. Effectiveness of sentinel lymph node intraoperative examination in 753 women with breast cancer: are we overtreating patients? Ann Surg 2012; 255: 976-80.
20. Nggada HA, Tahir MB, Musa AB, Gali BM, Mayun AA, Pindiga UH, et al. Correlation between histopathologic and fine needle aspiration cytology diagnosis of palpable breast lesions: a five-year review. Afr J Med Med Sci 2007; 36: 295-8.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: