
Durre-Samin Akram ( Honorary Chairperson, Health, Education and Literacy Programme (HELP), Pakistan; Former Chairperson of the Department of Pediatrics, Dow University of Health Sciences, Karachi, Pakistan. )
Yasmeen Suleman ( Senior Programme Manager, HELP, Karachi, Pakistan. )
Hafsa Mohammed Hanif ( Department of Pediatrics, Dow University of Health Sciences, Karachi, Pakistan. )
March 2016, Volume 66, Issue 3
Original Article
Abstract
Objective: To evaluate the efficacy, cost-effectiveness and acceptability of a \\\'high-density diet made from indigenous ingredients.
Methods: The retrospective study was carried out from September 2009 to May 2010 in District Sanghar, Sindh, Pakistan. A field office was established and staff was recruited and trained. A baseline survey was done to screen for malnourished children aged 6-23 months using mid-upper arm circumference, for which a cut-off value of 115mm was adopted. The screened children with a weight-for-height z score <-3 were registered and were supplied the high-density diet and micronutrients. Their mothers were counselled on infant and young child feeding practices.
Results: The mean age of 123 children in the study was 15.5±8.5 months, and mean weight was 5.91±1.18kg. Overall, 85(69%) children attained the target weight in a mean duration of 5.08±3.2 months. Besides, 29(23.5%) children were gaining weight, but had not achieved the target by the end of the study. The mean rate of weight-gain of children who recovered was 3.30±3.59 g/kg/day. No significant adverse effects were noted. There was no documented refusal of the therapeutic supplement. The net cost of rehabilitating a child was $34.31.
Conclusion: The high-density diet was reasonably efficacious in improving the nutritional status of severely malnourished children.
Keywords: Community-based therapeutic care, High-density diet, High-density food supplement, Malnutrition, Ready-to-use therapeutic food, Severe acute malnutrition. (JPMA 66: 251; 2016)
Introduction
In the backdrop of devastating floods in Pakistan, economic insecurity, political turmoil and deteriorating law and order situation, Pakistan has plunged into a critical state of child malnutrition. In 2010-11, nearly 15.1% of all children under 5 in the country were wasted, \\\'critical\\\' (>15%) by World Health Organisation (WHO) standards.1,2 Findings of the Flood Affected Nutrition Survey in Sindh, conducted in 2010 by the Department of Health in collaboration with United Nation International Children Education Fund (UNICEF), were even more striking, with 22.9% of all children aged 6-59 months in flood-affected areas wasted, and 6.1% severely so.3 In children under 5 years of age, malnutrition is defined by weight-for-age, height-for-age, or weight-for-height of <-2 standard deviation (SD) (of the WHO Child Growth Standards median), conditions termed underweight, stunting and wasting, respectively.2
Severe acute malnutrition (SAM) can be anthropometrically diagnosed by two criteria: weight-for-height <-3 SD of the WHO standards, or mid-upper arm circumference (MUAC) <115mm.4 WHO recommends that only severely malnourished children with complications should be admitted to a hospital, while those children with SAM who do not have complications should be managed in a community-based setting with ready-to-use therapeutic food (RUTF) and basic medical care, an approach referred to as community-based therapeutic care (CTC).4 It has been shown that in resource-poor settings, CTC can be highly effective, and has better outcomes compared to in-patient treatment.5 Further, the CTC approach allows greater population coverage and may be more cost-effective.6 In Pakistan, RUTF, in the form of \\\'Plumpy Nut\\\' is widely used in the rehabilitation programmes of UNICEF and World Food Programme (WFP). RUTF is not being manufactured in the country, and has to be imported by donor agencies at a very high cost. Further, the acceptability of imported RUTF is suboptimal, maybe because people are not accustomed to feeding their infants a peanut-based food with an unfamiliar flavour.
We formulated a high-density diet (HDD) (brand name: Nutri Help), which is a high-calorie food supplement manufactured using indigenous ingredients (gram powder, rice powder, milk powder, sugar and oil). The supplement can be consumed as such or mixed with varying amounts of water to generate a consistency of \\\'halwa\\\', \\\'kheer\\\' (traditional desserts with semi-solid and gruel-like textures, respectively) or a liquid drink, allowing it to be prepared in the form of dishes that local people are well acquainted to. Furthermore, the supplement has a pleasant, sweet taste, and by varying its consistency it can be consumed by both very young and relatively older children.
We used the supplement in certain pilot projects to assess its efficacy and acceptability. In a peri-urban settlement of Karachi, \\\'Khuda Ki Basti\\\', 24 severely malnourished children were identified and treated using the diet. Of them, 21 (87.5%) children attained the target weight (>-1 SD) within 3-4 months.6 We improved the HDD formula to enhance its composition and shelf life. In Tharparker, a district in rural Sindh, the enhanced diet was used to rehabilitate 611 malnourished children, as a component of a Gavi-funded project on \\\'Mother and Child Friendly Community\\\' (yet unpublished).Nearly 85% of the treated children attained the target weight in a mean span of 3-5 months. The product was also distributed to more than 1,900 children under 5 years of age in flood relief camps under a programme on \\\'Emergency Rehabilitation of Severely Malnourished Children\\\'. During this programme, carried out from September 2010 to February 2011, we found the supplement to have high acceptability. During the same period, the supplement was used in an alliance with Pakistan Paediatric Association as supplementary food for around 1,000 children in flood relief camps.
The current study was planned to assess the efficacy, cost effectiveness and acceptability of the supplement in a rural setting.
Subjects and Methods
The retrospective study was carried out from September 2009 to May 2010 and entailed analysis of data from a community-based therapeutic feeding programme (CTFP) to rehabilitate severely malnourished children. The study was not required to be reviewed by any ethical board in Pakistan as it was approved and funded by South Asia Regional Development Marketplace, World Bank. The project was implemented in two union councils of taluka Shahdadpur, District Sanghar, in rural Sindh. The two union councils, Jatia and Sarhari, have a population of 36,725 and 34,762, respectively. A field office was established and preliminary meetings with relevant government and non-government organisation (NGO) officials were held. Existing government personnel, including Lady Health Supervisors (LHSs) and Lady Health Workers (LHWs), were inducted as field workers. A series of training workshops were conducted for the capacity building of project employees at a secondary care hospital and 3 primary healthcare (PHC) centres in the area. The stabilising/therapeutic centre in the secondary care hospital and PHC centres were equipped with the following items for the assessment and monitoring of growth and nutritional status of children: infant weighing machines, height charts, MUAC measuring tapes for children and adults, infantometers, electric blender, digital weighing machine, hand mixers, mixing bowls, measuring spoons, measuring cups and jugs. The project staff was also given MUAC measuring tapes.
A proforma was designed for the baseline survey and was field-tested. A baseline survey of 1840 households was carried out in the study area to identify severely malnourished children using MUAC. The baseline survey screened for all children aged 6-23 months with a MUAC less than 115mm. The project supervisor verified the findings of the survey by visiting randomly selected households. Malnourished children identified by the survey were visited in their respective villages by a team comprising a doctor, LHS, LHW and project supervisor each. The team examined the nutrition status of the children using weight-for-height standards, and children with a z score of <-3 based on WHO Child Growth Standards4 were registered for rehabilitation. Those children who were malnourished by MUAC standard<115mm, but not by the weight-for-height standard, were not enrolled. The children were also examined for oedema and other complications. The subjects were given a week\\\'s supply of HDD along with 7 sachets of \\\'Baby Active\\\' micronutrient powder, to be sprinkled on HDD or any other food the child consumed. \\\'Baby Active\\\' is the brand name of a multi-micronutrient powder (also known as \\\'sprinkles\\\') marketed by Greenstar Social Marketing, and approved by the Ministry of Health. The amount of HDD that a child required was determined by his weight using a standard of 100cal/kg/day, and a week\\\'s ration was calculated accordingly. The daily energy requirement of well-nourished infants aged 6-23 months is around 90-110kcal/kg7 while severely malnourished infants require 150-220kcal/kg/day during rehabilitation.8 In our programme, mothers were advised to continue breastfeeding and home-made supplementary feeds in addition to HDD. Therefore, we prescribed 100kcal/kg/day, presuming that infants will obtain an additional 80-90 kcal from other sources. Every week, the LHW in-charge of the child was required to visit the home and record weight and adverse effects potentially related to the supplement. She would then give the mother another week\\\'s ration, and counsel her on infant and young child feeding (IYCF) practices. Mothers were advised to ensure that a packet of HDD was consumed within 3 days of its opening and any supplement leftover beyond this period was to be discarded. The ration was discontinued when the child reached >-1 SD, based on WHO criterion for discharge.9 Support group meetings were organised to provide an interactive forum to LHWs to educate and counsel mothers regarding home food and to respond to their questions.
The project was monitored by the project supervisor and LHS. Monitoring teams from the head office in Karachi were sent to the implementing area five times during the project. The duration of implementation was 19 months, from November 15, 2009, to June 15, 2011. At all stages of the project, officials in the government and partner NGO were kept informed of its progress and operations through meetings with the project supervisor.
The data generated was analysed using SPSS 16.
The HDD we formulated is made from gram powder, rice powder, milk powder, refined sugar and hydrogenated vegetable oil. It does not contain preservatives or artificial flavouring agents, and has a sweet, pleasant taste. We employed the services of a private-sector company that manufactures dairy products to produce the HDD. It was packed in aluminium sachets, each containing 250g. The sachets were then coded with batch numbers, dates of manufacture and expiry and ingredients. It was packed in cartons containing 150 sachets. The shelf life of the product is 3 months; it should ideally be stored in a cool and dry place.
Every 100g of HDD provides 458kcal of energy, 17.6g fat, 71.3g carbohydrates, 8.2g protein and 0.3g of fibre, according to an analysis of the nutritional content of the HDD by Pakistan Council of Scientific and Industrial Research. Instead of artificially fortifying the HDD, micronutrient sachets were given separately. \\\'Baby Active\\\', the multi-micronutrient powder that was used, contains 300µg of Vitamin A, 300mg of Vitamin C, 12mg of iron, 5mg of zinc, 160µg of folic acid and 90µg of iodine.
Results
Out of 1,840 children in the baseline survey, 240(13%) were screened and identified as SAM by MUAC criterion (<115mm). Of these, 90(37.5%) were verified by weight-for-height standards. During the course of the project, 33 more children were identified as SAM. Thus, a total of 123 children formed the study population. Of them, 58(47.15%) were males and 65(52.85%) were females. Overall mean age was 15.5±8.5 months, and mean weight was 5.91±1.18kg. The patient-to-health worker ratio was 3.74:1.
One (0.8%) child\\\'s family migrated to another area and 3(2.4%) children\\\'s mothers were not compliant and they were not included. Five (4%) children died during the rehabilitation phase. A verbal autopsy from the family members was done and it was found that the causes of death were unrelated to HDD (electrocution, thalassemia, abdominal tuberculosis [TB], coeliac disease). Out of the remaining 114(92.7%) children, 85(69%) achieved the target weight (>-1SD) in a mean period of 5.08±3.2 months. Mean rate of weight gain of these children was 3.30±3.59 g/kg/day. The remaining 29(23.5%) children were gaining weight satisfactorily but had not achieved the target weight by the end of the project (Figure).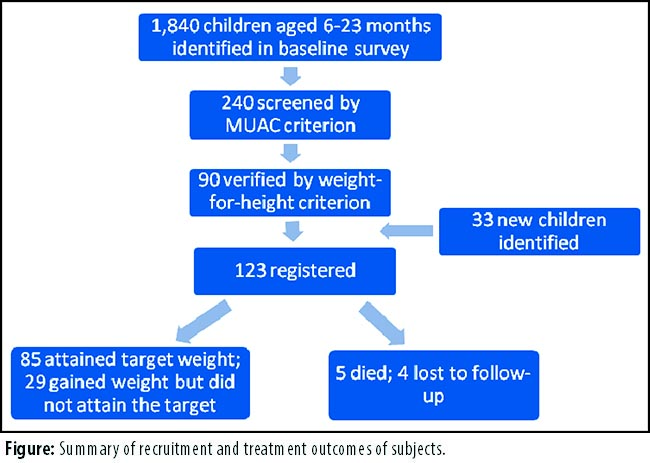
They were given a month\\\'s supply of HDD and micronutrients. No adverse reactions or issues concerning the acceptability of HDD and micronutrients were encountered. Indeed, during a monitoring visit, it was found that the siblings of malnourished children were also sharing the supplement. Therefore, midway during the project, the energy allocation was raised to 150cal/kg/day from 100cal/kg/day to compensate for the calories lost due to sharing by siblings.
The cost of manufacturing 100g of HDD was USD 0.22 (Rs20 [USD 1 = PKR 89.9 as of Jan 1, 2012]) and the net cost of rehabilitating a single child (including cost of HDD, micronutrients, transport, parental counselling and monitoring) amounted to USD 34.31 (Rs 3085).
Discussion
The outcome indicators of our programme are comparable to those of other studies in resource-poor countries that used RUTF for rehabilitation in a home setting. Ciliberto et al. studied the effectiveness of home-based therapy with RUTF in Malawian children in comparison to inpatient management at a health facility. In children being managed at home, 79% recovered, 3% died, 9.8% dropped out, and mean weight gain during the first 4 weeks was 3.5g/kg/day.10 The enrolment criterion in this study was children age 10-60 months, with a weight-for-height z score of <-2 or mild oedema or both, while recovery was deemed to have been attained when >-2 SD was reached. In another study on the home-based management of oedematous malnutrition with RUTF in 219 children, recovery rate in 8 weeks was 83%, fatality rate was 5% and mean weight gain was 2.8g/kg/day.11
Another study on home-based rehabilitation of severely malnourished children in a resource-poor setting in Delhi, India comprised children aged 6 months to 5 years with weight-for-height <70%. Home-based foods were used to provide 150 kcal/kg/day. The average weight gain was 3.2g/kg/day, which is comparable to our study.12
One study compared weight gains with RUTF, RUTF-supplemented local food and locally produced maize/soy dietary foods in home-based rehabilitation of severely malnourished children in Malawi. Human immunodeficiency virus (HIV) negative children <12 months with severe malnutrition were enrolled. Mean weight gain was 5g/kg/day in the RUTF group. However, it was 3.1g/kg/day in the RUTF supplemented and maize/soy groups, which is comparable to our study.13
During the course of the study it was found that siblings of malnourished children were sharing the supplement, due to which HDD allocation per child was raised to 150kcal/kg/day. To minimise food sharing, the Sindh Strategic Nutrition Response Plan proposes the provision of high-energy biscuits to siblings of a community-based management of acute malnutrition (CMAM) programme.14 It is likely that ration sharing by siblings had an adverse effect on recovery rate and the rate of weight gain. Besides, ration sharing is also indicative of a high acceptability of the product. Our therapeutic feeding programme and innovative product were thus fairly efficacious in improving the nutrition status of children.
Besides rehabilitating malnourished children, through our programme we also trained 2 LHSs, 42 LHWs, 2 LHVs and staff of the local hospital and Basic Health Unit (BHU) on CMAM, and IYCF. Further, the stabilising/therapeutic centres of a hospital, and 2 clinics were provided necessary equipment for the management of malnourished children. Maternal counselling on IYCF practices raised awareness, and to some extent, helped ensure sustainability of results. From the outset, we partnered with the government, and employed existing staff of the National Programme for Family Planning and Primary Healthcare, a strategy that had multifold benefits. Besides reducing implementation costs, it assisted in enhancing the potential sustainability of the programme and strengthening the government healthcare system. To optimise cooperation, government officials were involved in monitoring, progress reports were shared with them, and their contributions were recognised and appreciated.
Conventionally, imported RUTF (\\\'PlumpyNut\\\') has been used by UNICEF and WFP for the emergency rehabilitation of malnourished children following natural disasters in Pakistan and other parts of the world. One packet of \\\'PlumpyNut\\\' weighing 92g provides 500kcal (2,092kJ), equivalent to 5.4kcal/g.15 The energy density of our supplement is slightly less, 4.6kcal/g. The shelf life of \\\'PlumpyNut\\\' is 2 years, whereas that of our product is 3 months. Like \\\'PlumpyNut\\\', our product has a pleasant taste, and does not require refrigeration, preparation or reconstitution, in accordance with the definition of RUTF by WHO, WFP, UNICEF experts in 2007.7 Our HDD has the added advantage of having a flavour and consistency similar to a traditional dessert (\\\'halwa\\\'), and thus a high acceptability. The taste of \\\'PlumpyNut\\\', on the other hand, is relatively unfamiliar to children of the low socioeconomic class at whom rehabilitation programmes are directed.
Furthermore, our HDD is manufactured using indigenous, easily available ingredients. Therefore, it has the potential of a more widespread use if women are trained to prepare it in their communities. In our pilot interventional study in \\\'Khuda Ki Basti\\\', a local woman was trained to prepare HDD in her home.6 Community health workers would take it from her and supply it to the malnourished children being studied. Similarly, in the paediatric department of a large public hospital in Karachi, trained personnel have been preparing the supplement for malnourished in-patients since several years.
In addition, our study met most of the indicators outlined by SPHERE16,17 to measure the outcome of therapeutic feeding programmes. A clearly defined and agreed criterion for enrolment of children, dispensation of HDD and assessment and monitoring was established at the outset of the programme. Our coverage in rural areas was 58.8 % (ideal outcome >50%), proportion of exits from therapeutic care who died from causes unrelated to HDD was 4.1% (ideal outcome <10%), proportion of exits from therapeutic care who defaulted was 3.3% (ideal outcome <15%) and nutrition worker-to-patient ratio was 37.4% (ideal outcome >10%). Nutritional and medical care was provided according to internationally recognised therapeutic care protocols and equal emphasis was placed on breastfeeding, psychosocial support, hygiene, community outreach and clinical care. The discharge criterion used was attainment of weight >-1SD. However, our study did not meet the following outcome indicators: the minimum mean rate of weight gain in our study was 3.3g/kg/day (ideal outcome 8g/kg/day) and the proportion of children under therapeutic care who recovered was 69% (ideal outcome >75%).
As discussed above, other community-based interventions had similar rates of weight gain. Also, the children who were on this supplement at the completion of the project were gaining weight satisfactorily.
Conclusion
The therapeutic feeding programme was fairly well-designed with sound capacity building and counselling components, and a high nutrition worker-to-patient ratio. Further, the innovative HDD was reasonably efficacious in improving the nutritional status of severely malnourished children by way of a community-based approach. The supplement also had a high acceptability and was cost-effective in comparison to imported therapeutic foods. Since it is prepared using indigenous ingredients, its taste is more familiar to the local population, and it can be prepared not only in a factory but also by trained personnel in home and hospital settings.
Acknowledgements
We are grateful to the managers of National Primary Healthcare Programme and Sindh Agricultural and Forestry Workers Coordinating Organisation (SAFWCO) for their cooperation and valuable assistance. Thanks are also due to Dr. Mehak Muhammad Hanif, Research Assistant, HELP, for editorial assistance.
Conflict of Interest Statement: Dr. D. S. Akram is the founder and Honorary Chairperson of non-governmental organisation, \\\'Health, Education and Literacy Programme\\\' (HELP). The HDD was formulated for use at an inpatient therapeutic centre by her and Ms. Fatima Bharmal, a nutritionist. The therapeutic feeding project, on which this study is based, was devised and administered by HELP. The Emergency Rehabilitation programme in flood relief camps in which this diet has been used, was also a project of this organisation.
Dr. Yasmeen Suleman is the Executive Coordinator at Health Education and Literacy Programme (HELP). She was part of the implementation team of the Emergency Rehabilitation Programme.
Dr. Hafsa Hanif does not have any conflict of interest.
References
1. Pakistan Institute of Development Economics, Micro-nutrient Laboratories Aga Khan University and Medical Center Karachi. National nutrition survey 2010-2011. Planning Commission, Government of Pakistan and UNICEF. Islamabad: 2011
2. Nutrition Landscape Information System. Country profile indicators: interpretation guide. World Health Organization. Geneva: 2010
3. Department of Health, Government of Sindh. Flood-affected nutrition surveys: Sindh, Pakistan. DOH, Sindh. Karachi: 2010
4. WHO, UNICEF. WHO child growth standards and the identification of severe acute malnutrition in infants and children: A Joint Statement by the World Health Organization and the United Nations Children\\\'s Fund. World Health Organization, United Nations Children\\\'s Fund. Geneva, New York: 2009.
5. Sadler K. Community-based therapeutic care: treating severe acute malnutrition in sub-Saharan Africa [Ph.D thesis]. London: University College London; 2009.
6. Akram DS, Samad S, Arif F, Khan DS. Community based rehabilitation of severely malnourished children. J Pak Med Assoc 2010; 60: 179-81.
7. Experts of WHO, WFP, United Nations Standing Committee on Nutrition, UNICEF. Community based management of severe acute malnutrition: A joint statement by the World Health Organization, the World Food Program, the United Nations Standing Committee on Nutrition and the United Nations Children Fund. WHO. Geneva: 2007.
8. FAO, WHO, UNU experts. Energy and protein requirements: Report of a joint FAO/WHO/UNU expert consultation. World Health Organization. Geneva: 1985
9. WHO. Management of severe malnutrition: a manual for physicians and other senior health workers. World Health Organization. England: 1999
10. Ciliberto MA, Sandige H, Ndekha MJ, Ashorn P, Briend A, Ciliberto HM, et al. Comparison of home-based therapy with ready-to-use therapeutic food with standard therapy in the treatment of malnourished Malawian children: a controlled, clinical effectiveness trial. Am J Clin Nutr 2005; 81: 861-70.
11. Ciliberto MA, Manary MJ, Ndekha MJ, Briend A, Ashorn P. Home-based therapy for oedematous malnutrition with ready-to-use therapeutic food. Acta Paediatr 2006; 95: 1012-5.
12. SPHERE project team. The Sphere Project: Humanitarian charter and minimum standards in disaster response. 1sted. The Sphere Project. Geneva: 2000
13. Patel D, Gupta P, Shah D, Sethi K. Home based rehabilitation of severely malnourished children in resource poor setting. Indian Pediatr 2010; 8: 694-701
14. Manary MJ, Ndhekha MJ, Ashorn P, Maleta K, Breind A. Home based therapy of severe malnutrition with ready to use food. Arch Dis Childhood 2004; 89: 557-61
15. Nutrition Sector. Sindh Department of Health. Sindh Strategic Nutrition Response Plan. Department of Health; Sindh: 2011
16. Emergency items catalogue. The International Federation of Red Cross and Red Crescent Societies. Geneva: 2002; p 184.
17. SPHERE project team, The Sphere Project: Humanitarian charter and minimum standards in disaster response. 1sted. The Sphere Project; Geneva: 2000
18. SPHERE project team. The Sphere Project: Humanitarian charter and minimum standards in disaster response. 2nded. The Sphere Project; Geneva: 2004.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: