
Muhammad Hafeez ( Department of Medicine, Gastroenterology, CMH, Kharian Cantt. )
Asma Ansari ( Department of Gynecology and Obstetrics, CMH, Kharian Cantt. )
Saima Parveen ( Department of Gynecology and Obstetrics, Mohtarma Benazir Bhutto Shaheed Hospital, Mirpur, AK. )
Amjad Salamat ( Department of Medicine, Gastroenterology, Military Hospital, Rawalpindi. )
Anjum Aijaz ( Department of Medicine, Dermatology, CMH Malir Karachi. )
February 2016, Volume 66, Issue 2
Original Article
Abstract
Objective: To find out the frequency of intrahepatic cholestasis of pregnancy and its identification parameters.
Methods: The cross-sectional observational study was conducted in the Department of Medicine and the Department of Obstetrics, Combined Military Hospital, Kharian, from October 2013 to March 2014, and comprised all pregnant patients having symptoms suggestive of intrahepatic cholestasis which was confirmed after systemic inquiry, examination and biochemical analysis. Patients with cholestasis due to another reason, coagulopathies, thrombocytopenia and tumours were excluded. The patients were followed up till delivery to see the effects of cholestasis on mother and child.
Results: Out of 1001 obstetric patients, 31(3.1%) had intrahepatic cholestasis of pregnancy. Pruritus was the main symptom in 25 (85%) patients followed by rash in 20 (65%). In 20 (64%) patients, labour was induced. Mode of delivery was Caesarean Section in 18 (58%) patients and 9 (29%) had postpartum haemorrhage. Regarding neonatal complications, 22 (70%) required admission to neonatal intensive care and 15 (48%) had meconium aspiration.
Conclusions: A high frequency of intrahepatic cholestasis of pregnancy was observed. It had significant impact on maternal and foetal health.
Keywords: Intrahepatic cholestasis, Pregnancy liver problems, Prevalence of ICP. (JPMA 66: 203; 2016).
Introduction
Liver problems that women may have in pregnancy are preeclampsia, eclampsia, acute fatty liver of pregnancy, haemolysis, elevated liver enzymes, low platelet (HELLP) syndrome, and viral infections like hepatitis A, B, C, E, drug-induced hepatitis, connective tissue disorders, systemic lupus erythmatosis (SLE), auto-immune hepatitis, primary biliary cirrhosis, primary sclerosing cholangitis, Wilson\\\'s disease and Epstein-Bar virus infection. The exact cause of intrahepatic cholestasis of pregnancy (ICP) is not known, but environmental, genetic and hormonal factors are suggested to influence.1 Difference in prevalence in various parts of the world points to the environmental influence on the disease. Heterogeneous mutations in MDR3 (ABCB4) gene are reported in patients with ICP.2 In Caucasian ICP patients,16% such mutations have been demonstrated.3 ICP is more common in 3rd trimester when oestrogen levels are at peak.4 This concept is further strengthened by another study in which cholestasis was more in twins than in singleton pregnancies.5 Incidence of intrahepatic cholestasis is different in various parts of the world for unknown reasons.6 It is most common amongst women of Aurucanos in Chile.7 Very few studies have been carried out in this area probably because of expected low burden of the disease. Actually the situation is different and needs particular attention to prevent maternal and foetal complications that could be life-threatening if not identified. It was being observed that pregnant women present with intense itching in the third trimester of pregnancy. When their liver functions were carried out they were found to have intrahepatic cholestatic pattern after doing all other relevant investigations to rule out other causes. Pruritus was the main symptom which may be generalised but mostly it is on the palm and soles and happens at night. Due to intense itching, 80% patients have impaired quality of life. Sometime it is so distressing that it leads to insomnia and mental distress. Apart from the symptoms, ICP can lead to vitamin K deficiency, resulting in coagulopathy and postpartum haemorrhage.8 ICP may occur in 40-60% cases in subsequent pregnancies.9 Managing these patients is of paramount importance to reduce the maternal and foetal morbidity and mortality. Non-pharmacological management includes keeping patients well-hydrated, use of cotton cool and wearing loose clothes and avoiding high-fat diet. Antihistamines are usually not effective. Ursodeoxycholic acid is currently the only effective medicine in the dose of 10-15 mg/day in two to three divided doses to prevent maternal morbidity and perinatal complications.10 The drug should be given two to three weeks prior to delivery. Patient usually has relief within one to two weeks.11 Identification and treatment of these cases is vital as this is a disease of pregnant woman which changes pregnancy outcome.
The current study was planned to help general physicians (GPs), gynaecologists and obstetricians in picking up such cases for better maternal and child health.
Patients and Methods
The cross-sectional observational study was conducted in the Department of Medicine and the Department of Obstetrics, Combined Military Hospital (CMH), Kharian, from October 2013 to March 2014, and comprised all pregnant patients having symptoms suggestive of ICP which was confirmed after systemic inquiry, examination and biochemical analysis.
After obtaining approval from the institutional ethics committee, patients having symptoms suggestive of ICP were enrolled using consecutive purposive non-probability sampling. Patients with cholestasis due to another reason, coagulopathies, thrombocytopenia and tumours were excluded.
The patients included were interviewed in detail according to a structured proforma after taking informed consent. They were asked about their age, place of residence and if they had migrated from other cities, the duration since migration. For disease identification parameters, symptoms inquired were itching, colours of urine and stool, appetite, joint pains, rash, mouth ulcers or any other symptoms. History of diabetes mellitus and hypertension were also asked. Drugs that may lead to cholestasis, previous use of contraceptive pills and associated symptoms of cholestasis were also inquired. Any history of itching during the previous pregnancies and family history of intrahepatic cholestasis were explored. Detailed general physical and systemic examination was done. Investigations carried out were blood counts, urine examination, liver function tests, and viral serology like Hepatitis B surface Antigen (HBsAg), anti-hepatitis C Viral (HCV) antibodies, anti-hepatitis E Viral (HEV) and anti-hepatitis A Viral (HAV) antibodies. Other investigations were anti-nuclear antibodies (ANA), rheumatoid arthritis (RA) Factor, anti-mitochondrial antibodies (AMA), and abdominal ultrasound for any biliary duct dilatation. As serum bile acid concentration could not be performed because of the non-availability of the test anywhere in Pakistan, we kept ours a diagnosis of exclusion by symptoms and by performing other tests.
These patients remained under supervision of an obstetrician during antenatal period and they were followed up according to an antenatal visit protocol. Patients who needed intensive foeto-maternal monitoring were hospitalised. Delivery was planned and mode of delivery and postpartum haemorrhage frequency was noted. On delivery, number of babies admitted to the neonatal intensive care due to meconium aspiration was observed. Patients were followed up at 42 days postpartum to confirm resolution of clinical and laboratory parameters which is essential for diagnosing ICP.
All data was maintained and analysed on SPSS 21. Descriptive statistics were used and frequencies and percentages were calculated.
Results
Out of 1001 obstetric patients, 31(3.1%) had ICP with a mean age of 29.8±4.76 years. Mean age at presentation was 33.1±3.78 weeks and mean number of previous pregnancies was 2.5±1.36 (Table-1).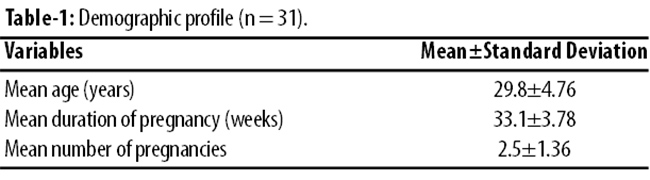
Overall, 90% patients belonged to the local area, while 10% were residents of other parts of the country but were living here for more than one year.
The main symptoms were itching over the body in 25 (85%) patients followed by rash 20 (65%). Frequency and percentage of signs and symptoms amongst the study population is shown in Table-2.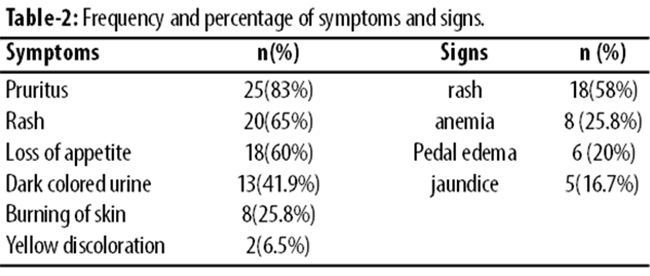
Three (10%) patients had ICP history in previous pregnancies, while 1(3.2%) patient had family history of ICP. One (3.2%) patient had developed itching during contraceptive use before pregnancy, and 2(6.5%) were using estalopram but this drug is not known to cause ICP.
Signs interpretation showed rash in 58%, jaundice 16.7%, pedal oedema 20% and anaemia in 25.8% patients. They were subjected to relevant Investigations (Table-3).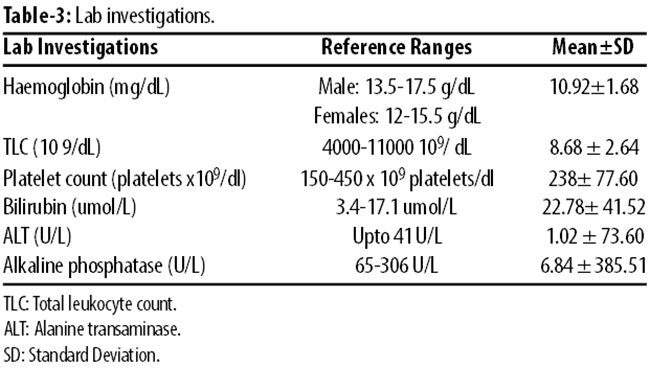
In 20 (64%) patients labour was induced between 37-38 weeks; mode of delivery was caesarean section in 18 (58%); 9 (29%) had postpartum haemorrhage (PPH); 22 (70%) neonates required admission to neonatal intensive care; and 15 (48%) had meconium aspiration.
Discussion
Incidence of ICP varies in different parts of the world as the cause is multifactorial, including genetics and environmental influences. Maximum incidence recorded is in Aurucanos in Chile 11%7 and 5.6% in primary Latin population in the United States.12 In a retrospective analysis of the prevalence of obstetric cholestasis carried out in the population of the south Birmingham area in various ethnic subgroups reported overall prevalence of 0.7% with an occurrence in the white population of 0.62%. In the Asians of Pakistani origin it was 1.46% and in the Asians of Indian origin it was 1.24%.13 There is a significant difference in incidence compared to our study\\\'s 3.1% that is almost double. This signifies the high prevalence in the study area which needs more investigations. One local study done in Rawalpindi had very low incidence of 0.4% but the risks of foeto-maternal complications was similar.14 In another study done in Karachi the incidence was 2% but the main concern were the cutaneous lesions as it was done by determatologists.15 There is difference amongst local and immigrant population in UK and the reported incidence is 0.7% in multi-ethnic population and 1.2-1.5% in Pakistani and Indian ethnic population.16 Pruritus was the main symptom that may be generalised but mostly it is on the palms and soles especially at night. In our study, itching was present in 83% followed by other symptoms. In a study done in India the incidence was markedly high 9% but the presentation was similar to our study. The study population was similar to ours and 66% were delivered by caesarean section mostly due to foetal distress and meconium aspiration, but surprisingly there were no neonatal sequale.17 ICP is a diagnosis of exclusion.18 Out of lab parameters, serum total bile acid (TBA) levels greater than 10 micromol/L is the most sensitive and specific marker. Though it is a sensitive marker, for the diagnosis and management of ICP there is no uniform agreement on the criteria. This is because of rapid turnover of the test every 3-4 days makes its management difficult, totally depending upon the bile acids. Every rise in micromol/L increases the foetal complication like spontaneous preterm labour, asphyxial events and meconium staining of the amniotic fluid.19 In another study maternal clinical and laboratory features, including elevated TBAs did not appear to be substantial predictors of foetal complications in ICP.12 Davis et al. suggested Alanine transaminase (ALT) as most sensitive marker in liver functions tests (LFTs)20 and Palma et al. used ALT and aspartate aminotransferase (AST) more than 40IU/L as partial criteria for the diagnosis of ICP.21 The recommended tests other than bile acid levels are transaminases, alkaline phosphatase, coagulation profile, and other investigations to rule out liver problems that pregnant patients may have. Laboratory investigations should be in conjunction with history and physical examination to make the final diagnosis. ICP is important to diagnose because of its implications for both foetus and mother. The reasons of the foetal complications related with ICP is not clearly known, but is considered to relate to an increased flux of bile acids into the foetal circulation. Foetal complications like meconium aspiration raised from 15% in general population to 58% in ICP patients like our study.22 Prematurity, perinatal mortality, respiratory distress syndrome, Neonatal Intensive Care Unit (NICU) admission were more than in general population,23 it was 66%, 22%, 70% and 41% respectively in our study. Respiratory distress syndrome was found twice as common in a study than in the general population compared to our study in which it was 41%.24
Managing these patients is of paramount importance to reduce the foeto-maternal morbidity and mortality. They were delivered either by induction or by Caesarean Section between 37 and 38 weeks as is current recommendation.16 Non availability of bile acids was a major limitation of our study but we adopted a pragmatic approach and diagnosed ICP like presently we are doing in our clinical setting by clinical features and excluding other causes. Bile acids were not measured in any of the local studies. The major contribution of this study is to create awareness about the burden of this disease in our country and to make way for further research. This could open avenues in finding out causes of many unexplained stillbirths and intrauterine deaths.
Conclusion
High frequency of ICP in this part of the country and identifying the disease timely needs special attention. The aim should be to educate the affected population and healthcare workers for better maternal and child health. This could be a cause of foetal distress and sudden unexplained intrauterine deaths. More studies in different parts of the country are required to find out the exact prevalence as this will prevent foetal and maternal complications if we know the exact burden of the disease. Also, there is need for making bile acid tests available for early and uniform diagnosis and making the process cost-effective.
References
1. Arrese M, Macias RI, Briz O, Perez MJ, Marin JJ. Molecular pathogenesis of intrahepatic cholestasis of pregnancy. Expert Rev Mol Med 2008; 10:e9.
2. Wasmuth HE, Glantz A, Keppeler H, Simon E, Bartz C, Rath W, et al. intrahepatic cholestasis of pregnancy : the severe form is associated with common variants of the of the hepato biliary phospholipid transporter ABCB4 gene. GUT 2007;56:265.
3. Bacq Y, Gendrot C, Perrotin F, Lefrau L, Ometfen S, Vie-Buret V, et al. ABCB4 gene mutation and single nucleotide polymorphism in women with intrahepatic cholestasis of pregnancy. J Med Genet 2009; 46:711.
4. Reyes H, Simon FR. Intrahepatic cholestasis of pregnancy: an estrogen-related disease. Semin Liver Dis 1993; 13:289.
5. Gonzalez MC, Reyes H, Arrese M, Figueroa D, Lorca B, Andresen M, et al. Intrahepatic cholestasis of pregnancy in twin pregnancies. J Hepatol 1989; 9:84.
6. Bacq Y. intrahepatic cholestasis of pregnancy. In Liver Dis 1999; 3:1.
7. Reyes H, Gonzalez MC, Ribalta J, Aburto H, Matus C, Schramm G, et al. Prevalence of intrahepatic cholestasis of pregnancy in Chile. Ann Intern Med 1978; 88:487.
8. Shornick JK. Dermatoses of pregnancy. Semin Cutan Med Surg.1998;17:172-81
9. Pathak B, Sheibani L, Lee RH. Cholestasis of Pregnancy. Obstet Gynecol Clin North Am. 2010;37:269-82.
10. Nichols AA. Cholestasis of pregnancy: A review of the evidence. J Perinat Neonatal Nurs. 2005;19:217-25.
11. Joshi D, James A, Quaglia A, Westbrook RH, Heneghan MA. Liver disease in pregnancy. Lancet. 2010;375:594-605.
12. Rook M, Vargas J, Caughey A, Bacchetti P, Rosenthal P, Bull R. Fetal Outcomes in Pregnancies Complicated by Intrahepatic Cholestasis of Pregnancy in a Northern California Cohort. PLoS One. 2012;7:e28343.
13. Abedin P, Weaver JB, Eggiton E. Intrahepatic cholestasis of pregnancy, prevalence and ethnic distribution. Ethn Health.1999; 4: 35-7.
14. Rasheed S, Afghan S, Mazhar SB. Whats fetomaternal outcome in patients with obstetric cholestasis. Ann Pak Inst Med Sci 2009; 5: 211-5.
15. Masood S, Rizvi D,Tabassum S, Akthar S, Alvi R. Frequency and clinical variants of specific dermatosis in third trimester of pregnancy: a study from a tertiary care centre. J Pak Med Assoc 2012; 62: 244-8.
16. Royal college of obstetricians and gynecologists. Obstetric Cholestasis. RCOG Green Top guidelines. no 43 April 2011.
17. Amita G, Tariia K, Yudhishtervir G, Yayoti H. Cholestasis of pregnancy. J Obstet Gynecol India 2009;59:320-32.
18. Saleh MM, Abdo KR. Intrahepatic cholestasis of pregnancy: review of the literature and evaluation of current evidence. J Women\\\'s Health (Larchmt). 2007; 16: 833-41.
19. Glantz A, Marschall HU, MattssonLA.Intrahepatic cholestasis of pregnancy: Relationships between bile acid levels and fetal complication rates. Hepatology. 2004; 40: 467-74.
20. Davies MH, da Silva RC, Jones SR, Weaver JB, Elias E. Fetal mortality associated with cholestasis of pregnancy and the potential benefit of therapy with ursodeoxycholic acid. Gut. Oct 1995; 37: 580-4.
21. Palma J, Reyes H, Ribalta J, Hernández I, Sandoval L, Almuna R, et al. Ursodeoxycholic acid in the treatment of cholestasis of pregnancy: a randomized, double-blind study controlled with placebo. J Hepatol.1997; 27: 1022-8.
22. Shaw D, Frohlich J, Wittmann BA, Willms M. A prospective study of 18 patients with cholestasis of pregnancy. Am J Obstet Gynecol. 1982; 142: 621-5.
23. Fisk NM, Storey GN fetal outcomes in obstetric cholestasis. Br J Obstet Gynaecol 1988; 95: 1137-43.
24. Zecca E, DeLuca D. Bile acid induced lung injury in newborn infants: a bronchoalveolar lavage fluid study. Pediatrics. 2008; 121: 146-9.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: