
Naila Azam ( Community Medicine Department, Army Medical College, Rawalpindi. )
Uzma Hassan ( Community Medicine Department, Rawal Institute of Health Sciences, Islamabad. )
Ayesha Farooq ( Community Medicine Department, Biochemistry Department, Foundation University Medical College, Rawalpindi. )
February 2016, Volume 66, Issue 2
Original Article
Abstract
Objective: To determine the effectiveness of intervention by education of doctors in improving the referral rate and quality in a public-sector healthcare setting.
Methods: The quasi-experimental study was conducted from March to September 2012 at PNS Rahat Hospital in naval sailors\\\' residential estate, Karsaz, Karachi. Two awareness sessions were held three months apart by a gynaecologist and a paediatrician. The sessions were aimed at communicating the consultant practice to female general practitioners employed at the two family welfare centres. Pre- and post-intervention data was collected manually from the record registers at the two centers as well as gynaecology and paediatrics outpatient clinics.
Results: The study comprised 10 female GPs. In paediatric clinic, there was 47% (118 post intervention/ 187 pre intervention) reduction in referrals for acute gastroenteritis and fever of unknown origin (32 post intervention/75 pre intervention). In gynaecology, 30% (50 post intervention/61 pre intervention) reduction was seen in referrals for severe anaemia in 2nd and 3rd trimesters of pregnancy, and an increase in referrals (35 post intervention/19 pre intervention) for high-risk cases indicating better counselling and case identification. Improved standard of counselling was also reflected by 31% reduced referrals (40 post intervention/ 58 pre intervention) for hyper-emesis gravidarum during the first trimester. The difference in referrals was not statistically significant (p>0.05) for paediatrics, but it was highly significant (p<0.001) for gynaecology.
Conclusion: Healthcare system can function optimally with focus on referral standards and by improving the communication between the primary care physicians and consultants.
Keywords: Healthcare system, Referral quality, Continued medical education, Communication. (JPMA 66: 174; 2016).
Introduction
The healthcare system in Pakistan is a three-tier system. The primary healthcare centres (PHCs) providing the essential healthcare staffed by general practitioners (GPs) or family physicians with their primary level paramedical staff attending to the majority of the population closer to their doorstep. These PHCs serve as the filter clinics for those requiring referral to the higher level of care by specialists located at the secondary or tertiary care hospitals.1,2
Health education of the population groups (dependent on PHCs) with stress on prevention of common public health problems (as outreach activities of PHCs), Identification of the common illnesses as they occur, their early management and timely identification of any complications requiring referral for specialist care is the mechanism of function and association requiring coordination and communication between the two levels of care; at organisational as well as physician levels.3 This practice of only essential and appropriately bona fide referrals to the higher level of care is the mainstay of an effective and efficient functioning healthcare system where the tertiary care facilities work as research and consultancy institutions with room for guidance to the PHC physicians.4,5 Primary care physicians are often confronted with overwork and insufficient time at their hands to offer effective consultation and convincing prescription to the patients. This leaves them with little or no time to review and catch up with newer protocols in primary healthcare, and often end up with in-efficient referrals causing strain on all the stakeholders, including the patients, cost of healthcare whether state paid or out-of-pocket private expenditure, the hospital systems and consequent overburden on the workforce at the receiving end in hospitals in the broader perspective.6,7 This brings to light the need for continued medical education (CME) and communication skills of primary care physicians with their colleagues in the higher levels of care.8,9
The GPs in a primary healthcare setting form the backbone of healthcare system. They interact with the higher levels of care through their referrals. Patients are referred to specialist care when investigation or therapeutic options are considered beyond the scope of primary care, and need for more specialised care is felt. A similar study was conducted in India to see the referral practices and outcomes in rural PHC and tertiary care setting respectively.10 Referral has considerable implications for patients, the healthcare system and healthcare costs. There is increasing awareness of a need to improve and fortify this process with a view to improving the quality of healthcare delivery, especially in the public sector. Australian healthcare trust has specially set up a task force to explore the importance and role of primary healthcare settings in promoting healthy lifestyles and preventing the increasing trends of chronic diseases.11 There has been focus on studying the effect of CME on practice performance of general and family physicians.12 The current study was planned to determine the effectiveness of CME intervention in doctors in terms of referral rate and quality in a public-sector healthcare setting.
Subjects and Method
The quasi-experimental non-randomised small-group study was conducted from March to September 2012 at PNS Rahat Hospital in naval sailors\\\' residential estate (SRE), Karsaz, Karachi. Two CME sessions were held three months apart by a gynaecologist and a paediatrician.
The quasi-experimental design was chosen because of the increasing trend of referrals to specialist outpatient departments (OPDs) from the PHCs for problems deemed as technically trivial or manageable at first level care as a routine activity. PNS Rahat hospital is a 160 bedded hospital with a single paediatrician consultant, who independently admits children to a 15-bed child ward when indoor care is deemed necessary. Similarly, the only gynaecologist sees the OPD as well as looks after a 25-bed gynaecology and obstetrics ward along with the labour room and operative requirements of the patients. The limited indoor bed capacity and trend of poorly managed but preventable problems necessitated this intervention.
The SRE at Karsaz includes the secondary level referral hospital, PNS Rahat and the two primary healthcare setups called the family welfare centres (FWCs) at Hanif SRE and Majeed SRE located within five kilometres of the hospital.
Data was collected at the two FWCs before and after the intervention. The first set of data for quarter ending March represented record from January to March 2012.
All the lady medical officers at the two FWCs, employed on contract by the naval medical authorities, comprised the study sample.
Karsaz, being a closed defence forces residential setup, has a documented resident population registered at each FWC as dependents.
In this setup, the term used for primary consultation is sick attendance/reporting as it is then included in facility work load documentation.
\\\'Referrals\\\' mean patients advised on refer form to consult the specialist in hospital OPD.
The CME sessions were conducted by the paediatric consultant for sharing views and giving guidelines for assessment and management of children at the outdoor clinic or subsequent referral to the hospital for specialist advice. The child specialist explained the referral pattern for paediatric cases from the primary clinic, especially withholding use of oral antibiotics for common cold and to stress on hand hygiene and oral rehydration therapy for the prevention and management of diarrhoea. Moreover, early recognition of signs of malnutrition, impending respiratory distress during acute respiratory infection (ARI) and moderate to severe dehydration after acute gastroenteritis were also discussed. He also explained the importance of follow-up and feedback by improving two-way communication between the two levels of healthcare.
Similarly, a consultant gynaecologist held two education sessions with the GPs to give guidelines for the assessment of obstetric cases for a more coordinated and systematic approach to referral for consultant advice. The gynaecologist also shared the importance of early but surely justified referrals by discussing the threshold of management at primary care level before having to consult at a specialist. She had prepared standing procedures and tips for management of common problems in pregnancy. These standard operating procedures (SOPs) stressed on managing complaints of early threatened abortion by counselling at PHC level and advice for rest at home as for hyperemesis gravidarum where simple dietary modifications are effective remedies. The intervention was further assessed by interview with the paediatric consultant and the gynaecologist. The quality and number of referrals to the paediatrics and gynaecology/obstetrics OPDs at PNS Rahat after six months were assessed for any change after the CME intervention.
The change in referral practices by identifying paediatric cases capable of management at primary care level and managing pregnancy and its related issues at primary care level like anaemia in pregnancy and hyperemesis while promptly referring high-risk cases for specialist care were indirectly measured by frequency of referred cases in the two specialist OPDs and the differential in referral pattern of cases was taken as an indicator of improved quality of practices. A special indicator of improved obstetric care was taken as frequency of Caesarean Section (CS) and emergency blood transfusions.
The intervention comprised two interactive sessions each by gynaecologist and paediatrician. There was no quantitative research questionnaire. The hospital OPD and PHC records were used for comparison. Paired sample before and after t-statistical test was applied. Descriptive analysis of data was also done.
Results
The study comprised 10 female GPs with mean professional experience of 10±5 years. The healthcare setup of the two FWCs and the details of the dependent population and sick attendance during the study period were noted (Table-1).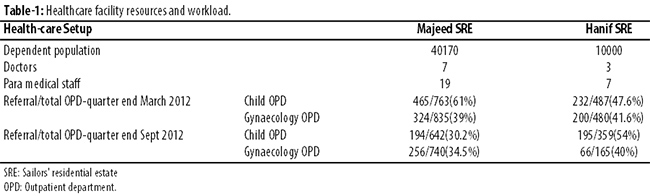
Interview with the paediatric consultant regarding quality of referrals revealed a trend of more detailed work-ups, children with definite physical findings and withholding antibiotics in prescription for minor cough and cold was observed. There was also an improvement in identification of high-risk obstetric cases and their timely referral to hospital with detailed counselling by the referring physician. There was an overall reduction in number of referrals per OPD day after the CME sessions.
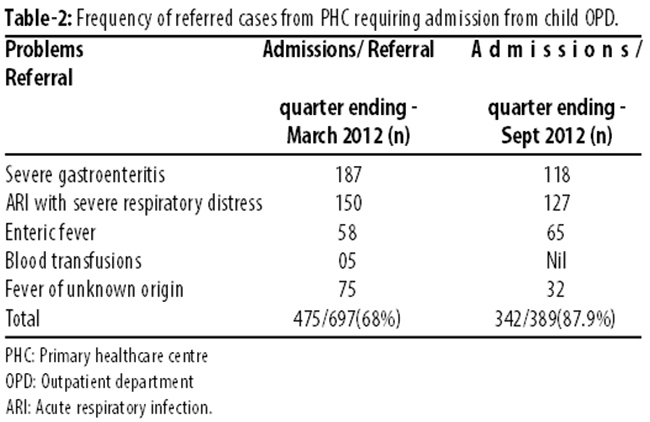
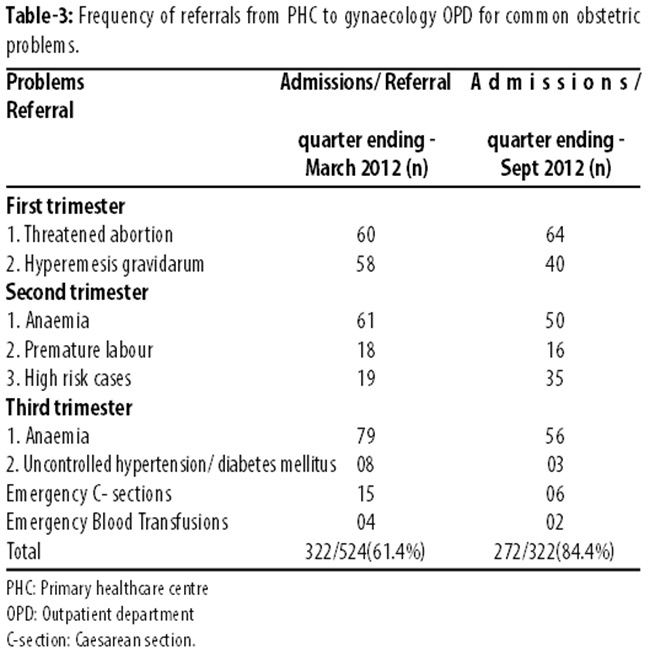
Data analysis at PNS Rahat Paediatrics Department (Table-2) and Gynaecology Department (Table-3) with regards to the operational definition of improvement in referral pattern reflected by the change in statistics of the two departments in selected parameters revealed around 47% reduction in referrals (118 post intervention/ 187 pre intervention) to paediatric OPD for acute gastroenteritis and fever of unknown origin (32 post intervention/75 pre intervention). In gynaecology OPD, 30% reduction in referrals for severe anaemia both during 2nd and 3rd trimesters (50 post intervention/61 pre intervention) and an increase in referrals for high-risk cases (35 post intervention/19 pre intervention) was seen, indicating better counselling and identification. Improved counselling was also reflected by 31% reduced referrals (40 post intervention/ 58 pre intervention) for hyperemesis gravidarum during the first trimester.
For paediatrics OPD, the difference was statistically non-significant (p>0.05). For the Gynaecology and Obstetrics OPD, the difference was highly significant (p<0.001).
Discussion
A look at the change in frequency of paediatric cases referred for common problems like acute gastroenteritis, ARI, severe anaemia and fever of unknown origin deemed fit by the child specialist to be admitted for indoor care reveals a 28% decrease in the total number of admissions though the dependant population parameters remained the same. This may be attributed to the improvement in outdoor management and primary level counselling by the doctors in the light of guidelines provided by the child specialist. Similar result has been reported in another study.9,13 Health education has been recognised as the main tool for the prevention of sanitation-related problems, including prevention strategies for most faeco-oral problems in lower middle class communities.14 Counselling rather than prescription of antibiotics as the preferred choice for primary care physician is also the recommended option15 Counselling for effectively exclusive breastfeeding and right nutrition with a balanced diet can be expected to substantially reduce the frequency of childhood anaemia and subsequent blood transfusions.14
The profile of referred cases in various trimesters of pregnancy to the gynaecology OPD also depicted a change in pattern of the complaints for referral; 17% reduction in referred cases, which matches well with similar studies conducted previously.16-18 In the first trimester of pregnancy, the most common complaint for referral is threatened abortion. This requires a lot of counselling and communication skills by the primary care physician to convince the woman about the nature and prognosis of the problem which is mostly under the patient\\\'s own control if she agrees to take adequate rest at home and relaxes mentally as well as physically. The same holds true for hyperemesis gravidarum cases. It also depends on a responsible and confident primary care physician who manages to hold back the patient before being considered serious enough to be referred to hospital for indoor management.19 Pregnancy-associated iron deficiency anaemia deemed serious enough to be referred to the hospital for either parenteral iron therapy or, worse, blood transfusion in the second or third trimester is another indicator of poor dietary counselling skills in the primary care centre for all females in the reproductive age group in general and pregnant ladies in particular, specially with reference to compliance with oral iron therapy. Most primary physicians fail to address the coping techniques for common side effects of the oral iron therapy.20 Patients landing up in hospital for emergency CS or uncontrolled hypertension or diabetes is another indicator of communication gap between the patient and primary care physicians who need to play a continued role in ensuring compliance by the patient with the consultant\\\'s advice and reducing the losses to follow-up in the consultant OPD to minimal.20 A reduced number of such referrals were also observed as an improvement in the practice of primary level clinics.21
It is recommended that an active coordination centre may be established in the referral hospitals which may keep an active track record of the disposal of all referred cases from the respective primary care centres. It should coordinate regular communication/feedback sessions for the consultants and the referring physicians. This would ensure a continuous updating of the referring practices and a conscious effort by the primary care physicians to keep up with emerging medical knowledge.
Conclusion
The healthcare system can function optimally with focus on referral standards and by improving the communication between the primary care physicians and consultants.
References
1. Soumerai SB, McLaughlin TJ, Avorn J. Improving drug prescribing in primary care: a critical analysis of the experimental literature. Milbank Q. 1989; 67:268-317.
2. Irby DM. Teaching and learning in ambulatory care settings: a thematic review of the literature. Acad Med. 1995; 70:898-931.
3. Sibille K, Greene A, Bush JP. Preparing physicians for the 21st century: Targeting Communication Skills and the Promotion of Health Behaviour change. Ann Behav Sci Med Educ. 2010; 16:7-13.
4. Viniegra VL. The path of criticism and education. Rev Invest Clin. 1996; 48:139-58.
5. Viniegra VL. Progress in medicine. Rev Investig Clin Organo Hosp Enfermedades Nutr. 1994; 46: 149.
6. Oxman AD, Thomson MA, Davis DA, Haynes RB. No magic bullets: a systematic review of 102 trials of interventions to improve professional practice. CMAJ. 1995; 153:1423-31.
7. U.S National Library of Medicine. Prenatal care [Online] 2012. [ cited 2000 Dec 13]. Available from: URL: http://www.nlm.nih.gov/medlineplus/prenatalcare.html.
8. Davis DA, Thomson MA, Oxman AD, Haynes RB. Evidence for the effectiveness of CME: a review of 50 randomized controlled trials. JAMA. 1992; 268: 1111-7.
9. Headrick LA, Neuhauser D, Schwab P, Stevens DP. Continuous quality improvement and the education of the general list physician. Acad Med. 1995; 70:S104-9.
10. Isaacs AI, Varghese N, Phillips CA, Plickal GG, Lhmar C. Outcome of referrals from a primary health institution in rural Karnataka. Pak J Med Sci. 2008; 24: 157-60.
11. Harris M. The role of primary health care in preventing the onset of chronic disease, with a particular focus on the lifestyle risk factors of obesity, tobacco and alcohol. Commissioned paper for the National Preventive Health Taskforce. (Online) 2009 (Cited 2015 Jan 16). Available from URL: http://www.preventativehealth.org.au/internet/preventativehealth/pulishing.nsf/content/OFBE203C1C547A82CA257529000231BF/file/commpaper-primary-hlth-care-harris.pdf.
12. Moattari M, Yadgari D, Hoseini SJ. The evaluation of a composed program of continuing medical education for general practitioners. J Adv Med Educ Prof. 2014; 2:120-5.
13. Gutiérrez G, Guiscafré H, Bronfman M, Walsh J, Martínez H, Muñoz O. Changing physician prescribing patterns: evaluation of an educational strategy for acute diarrhea in Mexico City. Med Care. 1994; 32:436-46.
14. Organization WH, others. The management of acute respiratory infections in children: practical guidelines for outpatient care. [Online] 1995 [Cited 2015 Jan 16]. Available from: URL: http://apps.who.int/iris/handle/10665/41803
15. Libreros V, Guiscafré H, Tomé P, Reyes H, Pérez Cuevas R, Gutiérrez G, et al. Patterns of therapeutic prescription in diarrhea and acute respiratory infections in 2 health care institutions: SS and IMSS. IV Characteristics of the medical prescriptions. Gaceta médica de México. 1992; 128: 505-52.
16. Pérez-Cuevas R, Guiscafré H, Muñoz O, Reyes H, Tomé P, Libreros V, et al. Improving physician prescribing patterns to treat rhinopharyngitis. Intervention strategies in two health systems of Mexico. Soc Sci Med. 1996; 42:1185-94.
17. Libreros V, Guiscafré H, Tomé P, Reyes H, Pérez Cuevas R, Gutiérrez G, et al. Patterns of therapeutic prescription in diarrhea and acute respiratory infections in 2 health care institutions: SS and IMSS. Gac Médica México 1992; 128: 505-52. Repeat reference # 15
18. Reyes H, Guiscafré H, Muñoz O, Pérez-Cuevas R, Martinez H, Gutiérrez G. Antibiotic noncompliance and waste in upper respiratory infections and acute diarrhea. J Clin Epidemiol. 1997; 50:1297-304.
19. Starfield B. Is primary care essential? Lancet. 1994; 344:1129-33.
20. Guiscafré H, Muñoz O, Padilla G, Reyes RM, González E, Bronfman M, et al. Strategies for improving the therapeutic patterns used in acute diarrhea in primary medical care units. VI. Evaluation of the strategy aimed at family physicians for increasing the use of oral rehydration and decreasing that of antibiotics and restrictive diets. Arch Invest Med (Mex). 1988; 19:395-407.
21. Guiscafre H, Martínez H, Reyes H, Pérez-Cuevas R, Castro R, Muñoz O, et al. From research to public health interventions. I. Impact of an educational strategy for physicians to improve treatment practices of common diseases. Arch Med Res. 1995; 26:S31-9.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: