
Yatan Pal Singh Balhara ( Department of Psychiatry, National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, New Delhi, India. )
Sanjay Kalra ( Department of Endocrinology, Bharti Hospital and B. R. I. D. E., Karnal, Haryana, India. )
October 2015, Volume 65, Issue 10
Primary Care Diabetology
Abstract
Diabetes and psychiatric disorders share a bi-directional relationship, with both affecting each other adversely. Just as achieving glycaemic control is important, so is ensuring that the person enjoys a good quality of life. All individuals with diabetes must be screened regularly for co-morbidity, especially depressive and anxiety disorders. Multiple evidence based psychotropic pharmacological interventions are available for management of these psychiatric disorders. Additionally, non-pharmacological interventions play a key role in comprehensive management of such patients.
Keywords: Anxiety disorders, Depression, Diabetes mellitus, Mental disorders, Primary health care.
Introduction
Primary care physicians have to take care of the person with diabetes as a whole. Just as achieving glycaemic control is important, so is ensuring that the person enjoys a good quality of life. Individuals diagnosed with diabetes are known to have poor quality of life. Co-occurring psychiatric disorders are important determinants of quality of life in individuals with diabetes.
Diabetes and Psychiatric Disorders
Diabetes and psychiatric disorders share a complex, bi-directional relationship, with both affecting each other adversely. Individuals diagnosed with diabetes have a higher prevalence of major depressive disorder, generalized anxiety disorder and eating disorders. Similarly, those diagnosed with major depressive disorders and schizophrenia are at higher risk of diabetes. The prevalence of major depressive disorder is twice among individuals with diabetes as compared to general population. Additionally, the risk of developing diabetes among individuals with depression has been found to be up to 60%.1 Diabetes is associated with greater frequency of suicidal thoughts and attempts.2
Impact of Psychiatric Disorders on Diabetes
Co-occurring psychiatric disorders among individuals diagnosed with diabetes are associated with poorer medication adherence, poorer compliance with diabetes self-care, higher functional impairment, poor glycaemia control, higher prevalence of complications, increased emergency room visits, higher frequency of hospitalization, and increased cost of medical care.3 It becomes imperative, therefore, to screen, diagnose, and manage these disorders as early as possible. The personal touch and close physician-patient bonding that characterizes primary care makes primary care practice the perfect platform to achieve this.
Screening and Diagnosis
All individuals with diabetes must be screened regularly for co-morbidity, especially depressive and anxiety disorders. Screening instruments and symptom check lists offer simple, less resource intensive way to identify those likely to be having psychiatric disorders. Patient health questionnaire (PHQ), and symptom checklist-90 (SCL-90) are examples of such instruments.4 The simplest tools for primary care are the Whooley 2-item questionnaire5 and the World Health Organization (WHO-5) questionnaire.6 Detailed diagnostic tools are also used in psychiatry, but are limited in utility in primary care settings due to time constraints.
Management
Motivational interviewing, stress management strategies, coping skills training, family therapy and collaborative case management can be included in primary diabetes care.7 Even the busiest physician can find time to offer "diabetes therapy by the ear", i.e., words of comfort.8
Multiple evidence based psychotropic pharmacological interventions are available for use. However, it is important to keep in mind the impact of such medications on glycaemic control.9 Medications for common disorders with lesser impact on glycaemia are listed in the Table.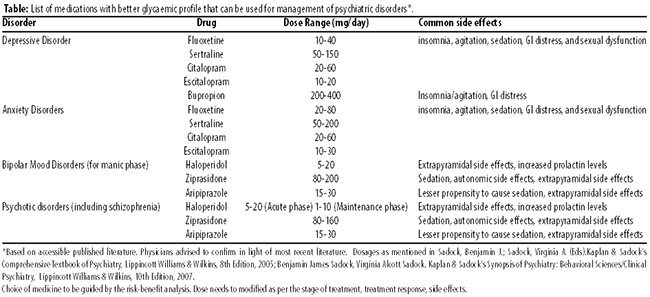
One must refer to a mental health professional in case of doubt.
Referral to Mental Health Professionals
Presence of moderate to severe psychiatric disorders, dependent use of psychoactive substance (such as alcohol and tobacco), progressive worsening of psychiatric symptoms, emergence of psychotic features, suicidal behaviour, requirement of pharmacological intervention for psychiatric problems warrant referral to psychiatrist.
References
1. Mezuk B, Eaton WW, Albrecht S. Depression and type 2 diabetes over the lifespan: a meta-analysis Diabetes Care, 2008, 31: 2383-2390.
2. Sarkar S, Balhara YS. Diabetes mellitus and suicide. Indian J Endocr Metab 2014;18:468-74.
3. Balhara YPS. Diabetes and psychiatric disorders. Indian J Endocrinol Metab. 2011; 15: 274-283.
4. Balhara YS, Kalra S, Das AK. Depression in diabetes: The need to screen. J Soc Health Diabetes 2013;1:51-2.
5. Whooley MA, Avins AL, Miranda J, Browner WS. Case-finding instruments for depression. Two questions are as good as many. J Gen Intern Med 1997;12:439-45.
6. WHO (Five) Well-Being Index (1998 version): Available from: http://cure4you.dk/354/WHO-5_English.pdf. Last accessed on 1 September 2014.
7. Kalra S, Sridhar GR, Balhara YP, Sahay RK, Bantwal G, Baruah MP, et al. National recommendations: Psychosocial management of diabetes in India. Indian J Endocrinol Metab. 2013;17:376-95.
8. Kalra S, Unnikrishnan AG, Baruah MP. Diabetes therapy by the ear. Indian J Endocr Metab 2013;17, Suppl S3:596-8
9. Balhara YS, Verma R, Kalra B. Pharmacological management of psychiatric disorders in pregnancy complicated by diabetics. J Soc Health Diabetes 2014;2:70-6.
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: