
Tabassum Zehra ( Department of Medicine, Aga Khan University Medical College, Karachi, Pakistan. )
Muhammad Tariq ( Department of Medicine, Aga Khan University Medical College, Karachi, Pakistan. )
Syeda Kauser Ali ( Department for Educational Development, Aga Khan University Medical College, Karachi, Pakistan. )
Afaq Motiwala ( Department of Medicine, Aga Khan University Medical College, Karachi, Pakistan. )
John Boulet ( Foundation for Advancement on International Medical Education and Research (FAIMER), USA. )
October 2015, Volume 65, Issue 10
Original Article
Abstract
Objective: To explore faculty\'s perceptions of challenges in providing verbal feedback to the Residents and suggest ways to overcome the barriers.
Methods: As part of a larger study on feedback assessment, five focus group discussions were conducted at the Department of Medicine, Aga Khan University Hospital, Karachi, during faculty development workshops held from January to June 2010. Qualitative grounded theory was used to explore faculty perceptions of challenges in providing verbal feedback to the Residents.
Results: Of the 54 faculty members, 49(91%) participated. Four themes that emerged were \'time constraint\' indicating high patient load; \'faculty related issues\' indicating faculty\'s apprehension about its own evaluation by Residents; \'educational issues\' indicating that the importance of feedback was not emphasised; and \'system and logistic issues\' indicating that the assessment form used for assessing Residents was ambiguous.
Conclusion: Work load of the faculty and the expectations with respect to patient care responsibilities may have an impact on the quality, timing, content and delivery of the feedback provided to the Residents.
Keywords: Feedback, Postgraduate medical education, Residents. (JPMA 65: 1069; 2015).
Introduction
Giving feedback is difficult and challenging, but providing timely feedback to the trainees is vital for their learning and it motivates the Residents in the process of competency achievements.1 It is accepted in literature that assessment, followed by feedback to the trainees, can provide an opportunity for in-depth analysis of their own performance, giving them an opportunity to reflect upon their strengths and weaknesses,1 allowing them to further enhance and build their capabilities and address deficient areas. Effective feedback should be based on direct observations, and should be specific and focussed. In any undergraduate or postgraduate educational institute, faculty is expected to provide regular feedback to the trainees.2 Based on literature, assessment should be based on competence (what the student or physician is able to do) and at the same time measure performance in real life situations (what he or she does in practice). Such experiential learning enables those being evaluated to learn from their own performance and improve accordingly.3-5 However, there is a general agreement in literature that giving feedback can be difficult5,6 and it has been reported that faculty may not feel comfortable in assessing trainees, especially when feedback relates to learning deficiencies.2 The questions with respect to feedback in postgraduate medical education are therefore related to challenges faced by the faculty in providing verbal feedback, and solutions to overcome the challenges.
Feedback which is constructive, appropriate, focussed and timely is a key strategy in teaching and learning.5 Busy clinicians believe that providing appropriate and timely feedback is a difficult task.5,6 Often they are constrained by patient care responsibilities, effectively decreasing their interaction time with the trainees. Trainees complain that feedback on their performance is often irrelevant or unclear, and sometimes even demoralising. It has also been reported that trainees are not given guidance as to how to use the feedback to improve subsequent performance.5,6
Literature suggests that the role of feedback is to identify strength and weaknesses, develop learning goals and thereby improve future performance.5,6 Literature also supports the concept of contextual learning where the learning is said to take place in an environment of increasing complexity of tasks. Meaningful engagement of residents in the learning context builds their capabilities through a transformation process which requires a feedback process about performances to know their areas of strengths/weaknesses without academic penalty.7
Faculty perspectives on providing feedback and residents\' satisfaction level regarding the teaching methodologies have been cited in literature.7,8 No studies were found in the local context which directly queried the faculty or the residents regarding the feedback process and the challenges faced.
A survey of Residents was conducted at the Department of Medicine, Aga Khan University Hospital, Karachi, which showed that even though informal feedback was provided to the Residents on various occasions, the implementation of regular and structured feedback was lacking. The Residents reported that only few faculty members gave feedback. The faculty perspective was not taken into account.
To better understand why the Residents were not receiving feedback, the current study was conducted to identify the challenges faced by faculty in assessing their trainees.
Subjects and Methods
The study comprised five focus group discussions (FGDs) that were conducted at the Department of Medicine, Aga Khan University Hospital (AKUH), Karachi, held from January to June 2010, after approval from the institutional ethical review committee.
Residents rotate through different specialties with assigned faculty for specified periods of time during the four years of Residency training. At the end of each rotation, an in-training record of assessments of each Resident in the domains of knowledge, skills and attitudes is submitted by the faculty member to the Residency programme director (PD). These forms are shared with the Residents at the end of each year of training.
The FGD method is used to explore a wide range of ideas and opinions of the participants on a well-defined topic. They lead to an in-depth conversation of the topic of interest with a small number of people and are widely used in qualitative research.9 The group members are selected based on their expertise, purpose of the FGD, and experience in the subject under discussion. The discussion leads to an in-depth overview of perceptions of the participants.9
Qualitative grounded theory research methodology was used to explore faculty perceptions of challenges in providing verbal feedback to the Residents. Grounded theory method is appropriate for exploratory research where the intent is to develop a theory \'grounded\' in the data to understand the process under study. Fundamental elements of the approach include an iterative process, theoretical sampling and data analysis using the method of constant comparison.10
A purposeful homogenous sampling of the faculty was done; all participants were faculty members with whom the Residents rotated during their Residency. The faculty was apprised of the purpose of the study and their consent was obtained. The FGDs were moderated and conducted by qualified medical educationists, including researchers. Each of the FGD lasted 30-45 minutes.
All fulltime faculty members were encouraged to participate in the group discussions, with each FDG having a minimum of 9 participants. Discussion was generated about faculty\'s perceptions of the purpose, process and demands of \'trainee feedback\'. Data was recorded verbatim by taking notes that were transcribed on flip charts. All the responses were kept confidential and anonymous.
Each focus group met with the same moderators. At the start of the session the moderators assured the faculty about the confidentiality. Moderator I opened the discussion by posing questions, while moderator II guided the group. Moderator III talked about feedback principles. All the three moderators were involved in asking the group about the challenges and their solutions.
The questions posed by the moderator I were: What do you know about feedback?; What experiences have you encountered while providing feedback?; What do you think are the challenges in giving feedback to the residents?; and what are your suggestions as solutions to the challenges stated/identified?
Discussion points were transcribed from the flip charts and observer notes. Moderators II and III separately reviewed all the transcripts after each session and coded the data under various headings. An analysis of words was done (word repetitions, key-indigenous terms, and key-words-in contexts) using an open coding technique. These codes and themes were then shared and any differences were sorted out and agreed upon by consensus. Any point that needed clarification was used as a guide for the next session. At the end of all sessions, four themes emerged from this process, which were then reviewed by Moderator I followed by a discussion with Moderator II till a consensus was reached on themes. The final report was written by Moderator III, circulated to the participant faculty for confirmation, and submitted to Moderator I and II for approval.
Results
Of the 54 faculty members, 5(9.2%) did not attend because they were either on leave or had prior clinical commitments. The response rate, as such, was 49(90.7%). The results of the five FGDs were summarised based on thematic categorisations. The four themes identified as challenges were: Time constraint; Faculty-related issues; Educational issues; System and logistic issues.
In terms of time constraint, all the five FGDs spontaneously and unanimously stated that, "time constraint of the clinical faculty is the most important factor that contributes to not providing timely and regular feedback". The "high patient loads in the clinics and involvement of faculty with the in-patient service leads to limited time to provide feedback to the residents".
1. As for the faculty-related issues, all members agreed that feedback is important and a key factor for Resident learning. However, 42(86%) participants stated that there is some apprehension regarding the provision of negative feedback which may ultimately reflect on their teaching dossier as low ratings by Residents on their evaluations. The same participants reported that they were not appropriately trained to provide feedback. Also, 11(22.4%) faculty members stated that since there is no incentive for the faculty on their involvement in the educational activities, they are reluctant to take time out from their clinical schedules.
2. When it came to educational issues, 28(57%) voiced their concern that the administration does not emphasise, or support, evaluation activities resulting in a lack of commitment by the faculty. Moreover, the faculty is not aware of the expectation from the Residents at different levels and the educational impact of giving feedback. This poses a problem since faculty\'s expectations of the Residents establish a standard and the difference between performance and the standard is what determines the content of the feedback.12 The faculty also felt that the expectations from the faculty are not clear to the Residents. Therefore, they are not able to identify levels of competence that they should achieve in the specialties by the end of each year.
3. System and logistic issues represented the last theme identified in FGDs. First-hand information is essential in providing feedback since insight into the actions can be obtained by direct observation of performance. Therefore, it is imperative to provide the feedback timely.
Faculty thought that the evaluation forms were not provided in a timely fashion to the faculty which means that the faculty had to remember the strong and the weak aspects of the Resident\'s performance. Faculty also felt that the form that is being used for Residents\' evaluation was very ambiguous and did not provide any space to mention the specific points for feedback.
The solutions suggested by the faculty to the challenges under each theme were noted separately (Figure).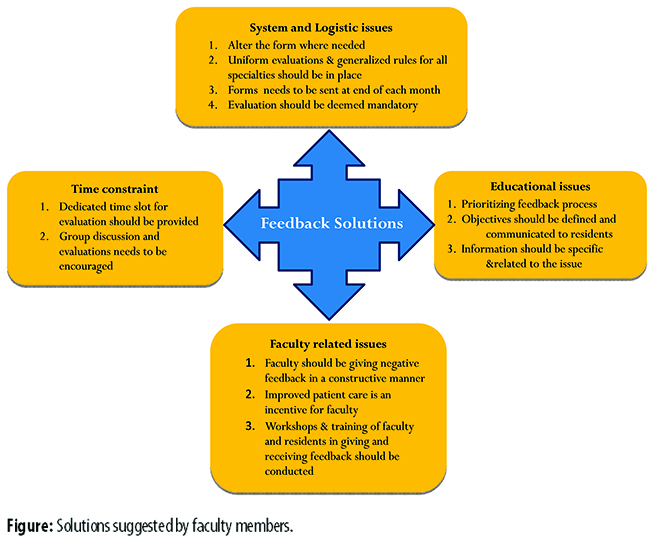
Discussion
Feedback is seen as an integral construct for many theories of learning and educational strategies. An understanding of the conditions for effective feedback both by the faculty and the Residents should facilitate both theoretical development and instructional practices.11-13
Professionals from undergraduate and postgraduate medicine agree that feedback is important in the development of expertise. Constructive feedback can reinforce good behaviour, allow for the correction of mistakes, and provide direction for improvement.12,13 Feedback is especially helpful for a \'trainee in difficulty\' who is at risk of failing due to deficiencies in knowledge, skills or attitudes.14,15
Measuring \'effectiveness of the feedback provided by the faculty\' requires clarity about the purpose of feedback. Feedback must be clear in order to judge the success of what it is trying to achieve. Therefore, the method and timing of measurement of the effectiveness will be dependent on the purpose.9 Similarly, a key factor in measuring effectiveness is who provides the feedback, the timeliness of feedback and a one-to-one environment.16-18
One of the main themes that were identified by the faculty was that dedicated time slot was not provided in their busy schedules for this purpose, and that the administration did not emphasise the importance of this activity. Participants were of the opinion that a dedicated institutional time slot should be provided to this activity. This has also been reported in other studies16,17 and provision of dedicated time has been considered an essential element to facilitate the process. According to the principles of feedback,16,17 in order to provide feedback, confidentiality as well as a friendly and supportive atmosphere should be maintained. The participants in the study suggested that the best reward for them would be improved patient care provided by the Residents. Timely and effective feedback to the Residents would enhance their training and, hence, their performances in patient care.
Faculty was reluctant to give feedback due to the fear of a negative emotional response and effect on their evaluation from Residents who receive negative feedback on performance. Therefore, they found it difficult to report unsatisfactory performance of the Resident. Literature supports the fact that faculty is reluctant to assign a failure grade to Resident on deficient performance due to its legal implications.13,14 The reluctance of the faculty to deliver feedback can also be attributed to a self-perceived lack of skill in observation and feedback.13,15 Most of the literature in education focuses on improving the delivery of feedback by the faculty. Though important, faculty believed that focussing on this alone will lead to less than optimal results. In order to reduce the fear of the faculty and enhance effective delivery, it is important to educate both the faculty and the Residents about the benefits of feedback and to train them in providing and receiving feedback respectively.14 The delivery of positive feedback may increase the likelihood that Residents evaluate the faculty member favourably, but this is not in the best interest of the Resident and must be understood by all faculty members. To avoid the scenario of negative impact on faculty evaluation, the Residents must receive information in a manner that enables them to accept it as non-evaluative and with the intention to improve clinical skills.
An important factor that contributes in not providing feedback is also not making appropriate records of the trainee performance.13 However, mechanisms ensuring timely documentation and appropriate documentation of such performances can help reduce the fear of the faculty in order to provide evidence-based feedback.13 In order to conduct a meaningful evaluation and to achieve improvement in performance as a result of the feedback provided, first-hand information is very important. Participants suggested that group evaluations, which may include the senior Resident and other faculty involved in teaching, should be conducted.
The faculty opined that Residents should be informed during the initial orientation that feedback will be a regular part of their Residency education. They should expect feedback at the end of every rotation and should not be surprised if delivered during patient care as well.18 Participants felt that the available administrative structures may be used to improve the implementation of the feedback process. A discussion of feedback during orientation will help ensure that the Residents differentiate feedback from evaluation, expect feedback, and even seek it out.18,19 It was agreed that evaluation of the Resident coupled with feedback should be deemed mandatory by the PD. There was a general agreement by the faculty that dealing with feedback as a learning opportunity helps the Resident to view the situation objectively.
System constraints in providing resources and faculty dissatisfaction with the system in place mean that the effectiveness of the feedback practices has never been considered important. It was agreed that the evaluation form should be modified according to the specialty needs and should be e-mailed to the faculty at the end of each month. There was also the agreement that a uniform process of feedback should be implemented across all disciplines of Medicine in the department.
Faculty development and an organised administrative structure can facilitate implementation of feedback system in the Residency programmes. Teaching students to receive feedback is an important educational technique that can contribute to the development of clinical skills as well. The faculty has less experience with giving oral feedback which can be improved by training.
The faculty preferred an anonymous form for assessing the Resident\'s competency and providing feedback, but they also valued face-to-face oral feedback. Facilitating effective face-to-face feedback encounters is essential to nurturing this critical skill from the beginning of Resident training.19-21 Faculty attitude is the key in helping Residents provide the feedback. A study conducted in the local context which reviewed feedback processes reported that the concept of providing and receiving feedback at any level in medical education in Pakistan is deficient and its significance with respect to teaching and learning is lacking.18
The limitation of the study is that it is a single-centre investigation so the results may not be generalised. Another limiting factor is that only faculty perspective was considered in the present study. Opinions of Residents and students on feedback could have enhanced the applicability of the perceived challenges. There is a need for wider application of the contextual environment of providing feedback and to investigate its effectiveness as potential area for further research. It can also be investigated that whether changes within the instructional strategies and responses to feedback provided does make a difference in Residents\' performance.
Conclusion
Contextual academic workload of the faculty and the university requirements with respect to patient care responsibilities may impact the quality, timing, content and delivery of the feedback provided. There is a need to streamline faculty training in providing verbal feedback, arranging dedicated time slots for feedback sessions by the faculty to the Residents, and conveying clear expectations to the Residents.
References
1. Assessment: Feedback to promote student learning, Teaching Development 2009. University of Waikato. [online] [Cited 2012 May 25]. Available from: URL: http://www.waikato.ac.nz/tdu/pdf/booklets/ 6_AssessmentFeedback.pdf.
2. Teaching and Learning Hub, Faculty of Medical and Health Sciences, University of Auckland. How do I make sure my feedback is timely and appropriate? [online] [Cited 2012 May 25]. Available from: URL: https://www.fmhshub.auckland.ac.nz/3_2.html.
3. Ronald M. Epstein MD. Assessment in Medical Education. N Engl J Med 2007; 356: 387-96.
4. Leach DC. Competence is a habit. JAMA 2002; 287: 243-4.
5. Poulos A, Mahony M. Effectiveness of feedback: the students\' perspective. Assessment Evaluation in Higher Education 2008; 33: 143-54
6. Watling C J, Lingard L. Toward meaningful evaluation of medical trainees: the influence of participants\' perceptions of the process. Adv Health Sci Educ Theory Pract 2012; 17: 183-94.
7. Fraser SW, Greenhalgh T. Coping with complexity: educating for capability. BMJ 2001; 323: 799-803.
8. Ali IS, Khan M, Khan A, Shah MF, Ali G. Trainees\' Feedback on the Prevailing Teaching Methods in Postgraduate Medical Institute, Lady Reading Hospital, Peshawar, Pakistan. J Coll Physicians Surg Pak 2012; 22: 317-9
9. Khan M E, Anker M, Patel BC, Barge S, Sadhwani H, Kohle R. The use of focus groups in social and behavioral research: Some methodological issues. World Health Stat Q 1991; 44: 145-9.
10. Watling, CJ, Lingard L. Grounded theory in medical education research: AMEE Guide No. 70. Med Teach 2012; 34: 850-61.
11. Bernard AW, Kman NE, Khandelwal S. Feedback in the Emergency Medicine Clerkship. West J Emerg Med 2011; 4: 537-42.
12. Price M, Handley K, Millar J, O\'Donovan B. Feedback all that effort, but what is the effect? Assessment Evaluation Higher Education 2010; 35: 277-89
13. Monica JM, Karel MS, McGaghie WC, Cate OJ. What is feedback in clinical education? Med Edu 2008; 42: 189-97.
14. McGraw R, Verma S. The trainee in difficulty. JCMU 2001; 3: 205-8
15. DudekNL, Marks B M, Regehr G. Failure to Fail: The perspectives of clinical supervisors Acad Med 2005; 80: S84-7
16. Sargeant J, Mann K. Feedback in Medical Education: Skills for Improving Learner Performance. In: ABC of Learning and Teaching in Medicine 2nd ed. Canada: Dalhousie University, Halifax; 2010
17. Bangert-Drowns R L, Kulik C C, Kulik JA, Morgan MT. The Instructional Effect of Feedback in Test-Like Events. Rev Educ Res 1991; 61: 213-38
18. Hattie J, Timperley H. The Power of Feedback. Review of Educational Research. Rev Educ Res 2007; 77: 81-112
19. Hamid Y, Mahmood S. Understanding constructive feedback: a commitment between teachers and students for academic and professional development. J Pak Med Assoc 2010; 60: 224-7
20. Lieb S. Carrie Ekey, Literacy Coaches Training. [online] 2012 [cited 2014 March 4]. Available from: URL: http://carrieekey.com/handouts/ Rotterdam2012/Eu_Coaches_Conf2_Rott_Day_1_A4.pdf
21. Ende J. Feedback in Clinical Medical Education. JAMA 1983; 250: 777-81.
Related Articles
Journal of the Pakistan Medical Association has agreed to receive and publish manuscripts in accordance with the principles of the following committees: